


Last Updated on January 13, 2026 by Nurseslab.in Editorial Team
Introduction
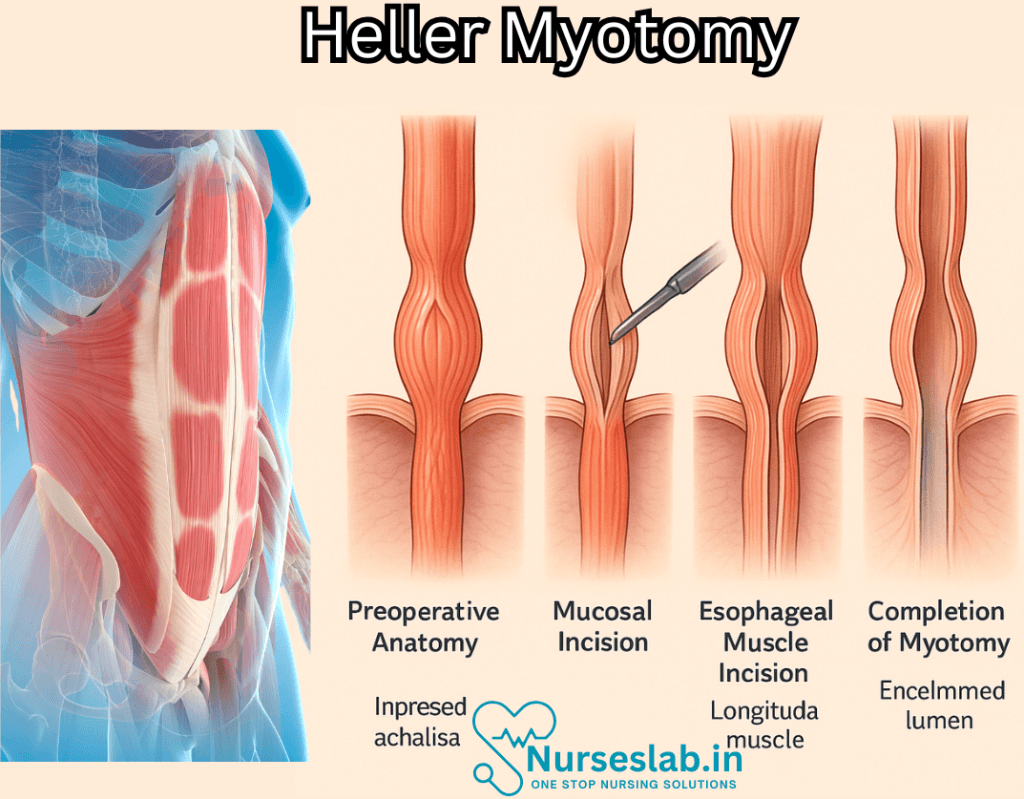
Heller Myotomy is a surgical procedure used to treat achalasia, a rare disorder of the esophagus that makes swallowing difficult. This condition occurs due to the failure of the lower esophageal sphincter (LES) to relax properly, causing a buildup of food and liquid in the esophagus. The procedure involves cutting the muscles at the LES to allow easier passage of food and liquid into the stomach.
History
The Heller Myotomy was first performed by Ernst Heller in 1913. Since then, the procedure has evolved significantly. Originally, it was an open surgery, but with advancements in medical technology, it is now commonly performed laparoscopically, which is less invasive and has a quicker recovery time.
Indications
The primary indication for a Heller Myotomy is achalasia, but it may also be used for other esophageal motility disorders. Symptoms of achalasia include difficulty swallowing (dysphagia), chest pain, regurgitation of food, and weight loss. When conservative treatments such as medication and pneumatic dilation fail, a Heller Myotomy is considered.
Preparation
Before undergoing a Heller Myotomy, patients typically undergo a series of diagnostic tests to confirm the diagnosis of achalasia and assess the function of the esophagus. These tests may include:
- Esophageal manometry: Measures the pressure and movement of the esophagus.
- Barium swallow: X-ray imaging to visualize the esophagus.
- Endoscopy: A flexible tube with a camera is inserted into the esophagus to examine it.
Procedure
The Heller Myotomy is usually performed under general anesthesia. During the laparoscopic procedure, small incisions are made in the abdomen through which a camera and surgical instruments are inserted. The surgeon then cuts the muscles at the LES, usually extending up to the esophagus and down to the stomach.
In some cases, a partial fundoplication, such as a Dor or Toupet procedure, is performed simultaneously to prevent gastroesophageal reflux disease (GERD). This involves wrapping the top part of the stomach around the lower esophagus to reinforce the LES and prevent acid reflux.
Recovery
Post-surgery, patients are monitored in the hospital for a few days. They may experience some pain and discomfort, which is managed with medication. Most patients can resume normal activities within a few weeks. A liquid or soft diet is recommended initially, gradually transitioning to solid foods.
Regular follow-up appointments are necessary to monitor the patient’s recovery and ensure the success of the surgery. In some cases, additional treatments or interventions may be required if complications arise.
Complications
While Heller Myotomy is generally safe, it carries some risks, as with any surgical procedure. Potential complications include:
- Esophageal perforation: A tear in the esophagus.
- GERD: Chronic acid reflux.
- Infection: At the surgical site.
- Bleeding: During or after the surgery.
It is important to discuss these risks with the surgeon before the procedure.
Outcomes
Heller Myotomy has a high success rate, with most patients experiencing significant improvement in their symptoms. Studies have shown that up to 90% of patients report relief from dysphagia and other related symptoms. Long-term outcomes are generally positive, although some patients may require additional treatments for GERD.
Nursing Care of a Patient with Heller Myotomy
Heller Myotomy is a surgical procedure used to treat achalasia, a condition characterized by difficulty in swallowing due to the inability of the lower esophageal sphincter to relax. Nursing care for patients undergoing Heller Myotomy is crucial in ensuring a smooth recovery and optimal outcomes. This guide provides an overview of the essential nursing care practices for such patients.
1.Preoperative Care
Patient Education
It is essential to educate the patient about the procedure, its benefits, and potential risks. Providing detailed information helps in reducing anxiety and promoting cooperation.
Nutritional Support
Patients may require nutritional assessments and modifications to their diet before surgery. A soft or liquid diet may be recommended to ensure adequate nutrition while minimizing discomfort.
Preparation for Surgery
Nurses should ensure that the patient has fasted for the required period before surgery. Preoperative medications may be administered as prescribed.
2.Postoperative Care
Pain Management
Administer prescribed analgesics to manage postoperative pain effectively. Monitor the patient’s response to pain medication and adjust the plan as necessary.
Monitoring and Assessment
Regularly monitor vital signs, including heart rate, blood pressure, and respiratory rate. Assess for any signs of complications such as infection, bleeding, or esophageal perforation.
Nutritional Care
Gradually reintroduce oral intake, starting with clear liquids and progressing to a soft diet. Monitor the patient for any difficulties in swallowing or signs of aspiration.
3.Prevention of Complications
Implement measures to prevent postoperative complications. Ensure proper wound care to prevent infection and monitor for any signs of esophageal perforation or GERD.
Patient Positioning
Encourage the patient to maintain an upright position, especially during and after meals, to facilitate swallowing and reduce the risk of reflux.
4.Long-term Care and Follow-up
Regular Follow-up Appointments
Schedule and remind the patient of regular follow-up appointments to monitor recovery and address any emerging issues promptly.
Ongoing Patient Education
Continually educate the patient about lifestyle modifications that can help manage symptoms and prevent complications. This may include dietary adjustments, avoiding heavy meals, and maintaining an upright position during meals.
Support Groups and Counseling
Encourage the patient to join support groups or seek counseling if needed. Emotional support is vital for coping with chronic conditions and surgery recovery
REFERENCES
- Arcerito M, Jamal MM, Perez MG, et.al. Esophageal Achalasia: From Laparoscopic to Robotic Heller Myotomy and Dor Fundoplication. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9355798/). JSLS. 2022 Jul-Sep;26(3): e2022.00027.
- Adriana Laser, Open Heller Myotomy Technique, Updated: Oct 02, 2024, https://emedicine.medscape.com/article/1965924-technique
- Cappell MS, Stavropoulos SN, Friedel D. Updated Systematic Review of Achalasia, with a Focus on POEM Therapy. https://pubmed.ncbi.nlm.nih.gov/31451984/). Dig Dis Sci. 2020 Jan;65(1):38-65.
- McCarthy E, Jao SL, Pryor AD. Laparoscopic Heller Myotomy and Dor Fundoplication (https://pubmed.ncbi.nlm.nih.gov/35597821/). World J Surg. 2022 Jul;46(7):1527-1530.
- Vaezi MF, Pandolfino JE, Yadlapati RH, et.al. ACG Clinical Guidelines: Diagnosis and Management of Achalasia. https://pubmed.ncbi.nlm.nih.gov/32773454/). Am J Gastroenterol. 2020 Sep;115(9):1393-1411.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


