


Introduction
Candida parapsilosis is a species of yeast that has rapidly ascended in medical relevance over the past few decades. Once considered a benign commensal organism, it is now recognized as a significant opportunistic pathogen, particularly in immunocompromised patients and those with indwelling medical devices. Its ubiquity, adaptability, and evolving resistance patterns make it a subject of growing interest within clinical microbiology and infectious disease circles.
Biology and Taxonomy
Classification:
- Kingdom: Fungi
- Phylum: Ascomycota
- Class: Saccharomycetes
- Order: Saccharomycetales
- Family: Debaryomycetaceae
- Genus: Candida
- Species: parapsilosis
Morphology and Growth:
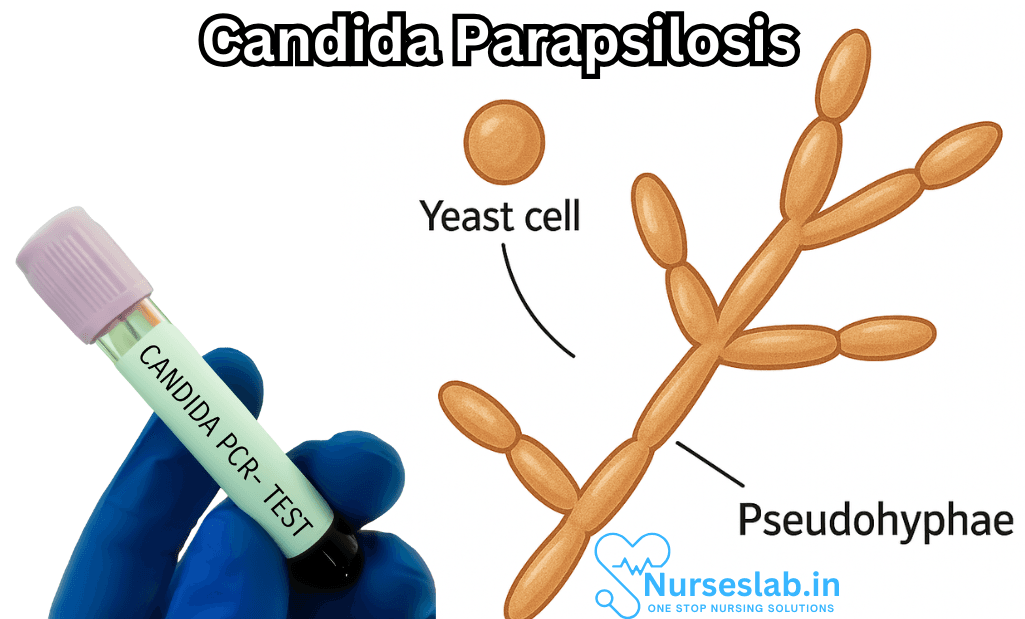
Candida parapsilosis is distinctive for its ability to grow as budding yeast cells, elongated pseudohyphae, and true hyphae in certain conditions. When cultured on Sabouraud’s dextrose agar, colonies usually appear smooth, creamy, and slightly lustered. Microscopically, it demonstrates oval or cylindrical budding cells and the formation of branched pseudohyphae—a feature that aids in its identification and distinguishes it from other Candida species.
Natural Habitat:
C. parapsilosis is found widely in nature. It resides on human skin, particularly in the subungual region (beneath the fingernails), and can also be isolated from soil, water, and the surfaces of plants. Its presence on the hands of healthcare workers is one reason why it is frequently associated with nosocomial (hospital-acquired) infections.
Clinical Significance
Emergence as a Pathogen:
In the past, Candida albicans was considered the predominant causative agent of candidiasis; however, the incidence of non-albicans Candida species, including C. parapsilosis, has grown. Advances in medical technology have inadvertently contributed to this shift, as the use of catheters, prosthetic devices, and parenteral nutrition creates new niches for colonization.
At-Risk Populations:
- Neonates (especially preterm infants)
- Patients with central venous catheters
- Individuals receiving total parenteral nutrition
- Immunocompromised hosts (e.g., those with HIV/AIDS, cancer, transplant recipients)
- Patients in intensive care units (ICUs)
Clinical Manifestations:
Candida parapsilosis is notorious for causing:
- Candidemia (bloodstream infection)
- Endocarditis (infection of heart valves)
- Peritonitis
- Urinary tract infections
- Wound infections
- Onychomycosis (nail infection)
Neonatal candidemia, in particular, is a grave concern due to the high morbidity and mortality rates associated with C. parapsilosis bloodstream infections in this vulnerable population.
Pathogenesis
Adherence and Biofilm Formation:
One of the defining features of C. parapsilosis is its robust capacity to adhere to plastic and other abiotic surfaces. It is a prolific biofilm former—an ability that renders it highly resistant to antifungal agents and host immune defenses. Biofilms are complex communities of yeast cells embedded in a self-produced matrix, which can develop on medical devices such as catheters and prosthetic heart valves, leading to persistent and difficult-to-treat infections.
Virulence Factors:
- Hydrolytic enzymes: Secreted aspartyl proteinases and lipases facilitate tissue invasion and nutrient acquisition.
- Dimorphic switching: The organism’s ability to alternate between yeast and pseudohyphal forms aids its survival and pathogenicity.
- Phenotypic plasticity: Adaptation to diverse environmental conditions, including temperature and nutrient fluctuations.
Diagnosis
Laboratory Identification:
Diagnosis of C. parapsilosis infection relies upon both culture and advanced molecular techniques. Blood cultures remain the gold standard for candidemia, but newer methods such as PCR and MALDI-TOF mass spectrometry allow for more rapid and accurate identification.
- Cultures: C. parapsilosis grows rapidly on standard fungal media, with colony morphology providing initial clues.
- Biochemical tests: Commercial kits may test sugar assimilation and enzyme activity to differentiate Candida species.
- Molecular diagnostics: DNA-based assays help confirm species identity, which is crucial for guiding therapy.
Treatment
Antifungal Therapy:
C. parapsilosis has unique susceptibilities compared to other Candida species. While azoles (such as fluconazole) are generally effective, there have been reports of reduced susceptibility in some isolates. Echinocandins (e.g., caspofungin, micafungin), which are first-line agents for candidemia, are less effective against C. parapsilosis due to intrinsic resistance mechanisms.
- Azoles: Common agents include fluconazole and voriconazole.
- Polyene antifungals: Amphotericin B remains an option, especially in severe cases.
- Echinocandins: Generally avoided unless no alternatives exist.
Device removal:
For device-associated infections, removal of the implicated catheter or prosthesis is often necessary to achieve cure, given the recalcitrance of biofilm-associated yeast to medical therapy.
Resistance and Epidemiology
Antifungal Resistance:
Emerging resistance is a growing concern. Mechanisms include alterations in target enzymes, efflux pump activity, and biofilm-mediated protection. Surveillance studies show geographic variability in resistance patterns, underscoring the importance of local epidemiology in informing therapy.
Global Distribution:
C. parapsilosis has a cosmopolitan distribution, with higher prevalence in certain regions such as Latin America and Asia. Hospital outbreaks have been linked to lapses in infection control, emphasizing the critical role of hand hygiene and aseptic technique in prevention.
Prevention and Control
Infection Control Measures:
- Strict hand hygiene practices for healthcare workers
- Proper management and prompt removal of indwelling devices
- Environmental decontamination, especially in ICUs and neonatal units
- Surveillance for outbreaks and resistant strains
Prophylactic Strategies:
Prophylactic antifungal therapy may be used in select high-risk populations, such as extremely low birth weight neonates, but must be balanced against the risk of fostering resistance.
Nursing Care of Patient with Candida Parapsilosis
Nurses play a pivotal role in the prevention, identification, and management of infections caused by this organism, ensuring optimal patient outcomes through vigilant assessment, targeted interventions, and effective patient education.
Nursing Assessment
Nurses must conduct thorough assessments to identify signs and symptoms of C. parapsilosis infection, monitor for complications, and evaluate the patient’s risk profile.
Initial Assessment
- History Taking: Identify risk factors such as recent hospitalization, use of invasive devices, immunosuppression, or recent surgeries.
- Physical Examination: Inspect for fever, chills, hypotension, erythematous or pustular lesions (especially around catheter sites), and signs of sepsis.
- Laboratory and Diagnostic Evaluation: Review blood cultures, complete blood count, inflammatory markers (CRP, ESR), and any imaging studies ordered by the medical team.
Ongoing Monitoring
- Monitor vital signs for fever, tachycardia, hypotension, and hypoxia.
- Observe insertion sites of catheters for redness, swelling, discharge, or other signs of local infection.
- Regularly assess for new or worsening symptoms, such as altered mental status, oliguria, or respiratory distress, which may indicate systemic involvement.
Nursing Diagnoses
Several nursing diagnoses may be relevant for the patient with Candida parapsilosis, including:
- Risk for infection related to invasive devices and immunosuppression
- Impaired skin integrity related to presence of lesions or indwelling devices
- Risk for fluid volume deficit related to fever and sepsis
- Acute pain related to infection or associated procedures
- Anxiety related to illness, isolation procedures, or invasive interventions
Nursing Interventions
Comprehensive nursing care involves both direct clinical management and supportive care tailored to the individual patient’s needs.
Infection Control
- Practice strict hand hygiene before and after patient contact.
- Implement standard and, if necessary, contact precautions to prevent nosocomial transmission.
- Use aseptic technique during insertion and maintenance of intravenous lines and catheters.
- Ensure timely removal or replacement of unnecessary invasive devices.
- Disinfect equipment and the patient’s environment regularly to minimize contamination.
Antifungal Therapy Support
- Administer antifungal medications as prescribed, which may include agents like fluconazole, echinocandins, or amphotericin B.
- Monitor for and promptly report potential side effects of antifungal therapy, such as renal dysfunction, hepatotoxicity, and infusion-related reactions.
- Assess for potential drug interactions and ensure dosage adjustments in renal or hepatic impairment.
- Ensure accurate timing and documentation of medication administration for optimal therapeutic effect.
Catheter and Device Care
- Perform daily assessment of all catheter and device sites for signs of infection.
- Follow institutional protocols for the care, cleaning, and dressing changes of central lines and other invasive devices.
- Collaborate with physicians to evaluate the necessity of continued device use and facilitate removal when possible.
Skin Integrity Maintenance
- Inspect skin regularly, especially in areas prone to moisture or breakdown.
- Keep skin clean and dry to prevent secondary infections.
- Apply barrier creams or protective dressings as needed, particularly around catheter sites.
Fluid and Electrolyte Management
- Monitor fluid intake and output vigilantly, especially in patients with fever or sepsis.
- Assess for signs of dehydration, such as dry mucous membranes, decreased skin turgor, or hypotension.
- Administer intravenous fluids as ordered and monitor for fluid overload, particularly in patients with renal impairment.
Pain and Fever Management
- Assess pain levels regularly and administer analgesics as prescribed.
- Monitor temperature and provide antipyretics as indicated.
- Offer non-pharmacological comfort measures such as cool compresses or relaxation techniques.
Monitoring for Complications
- Be alert for signs of systemic infection or sepsis, including hypotension, tachycardia, altered mental status, and multi-organ dysfunction.
- Report any sudden changes in the patient’s condition to the healthcare provider promptly.
- Assist in obtaining repeat blood cultures or additional diagnostic samples if the infection persists or worsens.
Patient and Family Education
Education is a cornerstone of nursing care and essential for both patients and their families to promote understanding, adherence, and prevention of future infections.
- Explain the nature of the infection, risk factors, and the rationale for treatment clearly and compassionately.
- Teach the importance of hand hygiene and infection control measures at home and in the hospital.
- Instruct on the proper care of indwelling devices and signs of infection to watch for after discharge.
- Discuss medication regimens, potential side effects, and the importance of completing the full course of therapy.
- Reinforce the need to keep follow-up appointments for monitoring and further care.
- Provide psychological support to reduce anxiety and answer any questions about isolation procedures or prognosis.
Collaborative Care
The management of Candida parapsilosis infection is multidisciplinary. Nurses coordinate closely with physicians, pharmacists, infection control teams, and other allied health professionals to ensure comprehensive care.
- Communicate effectively with the healthcare team regarding changes in the patient’s condition or response to therapy.
- Facilitate early identification and management of complications through interdisciplinary rounds and discussions.
- Refer to dietitians, social workers, or other specialists as needed based on the patient’s holistic needs.
Special Considerations
Neonates and Paediatrics’:
- Neonates, especially premature infants, are highly susceptible to C. parapsilosis infections, often via contaminated hands or devices.
- Nurses must ensure meticulous hand hygiene, maintenance of sterile technique, and close monitoring for subtle signs of infection in this population.
Immunocompromised Patients:
- Patients with malignancies, organ transplants, or HIV may require longer and more aggressive antifungal therapy.
- Frequent monitoring for drug toxicity and secondary infections is essential.
Prevention Strategies
Hospital-Based Prevention:
- Rigorous hand hygiene by all healthcare workers and visitors.
- Minimizing the use of invasive devices whenever possible.
- Implementing bundle care strategies for central lines to reduce catheter-related infections.
- Ongoing education for staff about the risks and prevention of fungal infections.
Community and Aftercare:
- Educate discharged patients and caregivers about signs of recurrent infection or complications.
- Support adherence to medication and follow-up schedules post-discharge.
REFERENCES
- Centers for Disease Control and Prevention (U.S.). Invasive Candidiasis Statistics. https://www.cdc.gov/fungal/diseases/candidiasis/invasive/statistics.html. Last reviewed 1/13/2023.
- Trofa D, Gácser A, Nosanchuk JD. Candida parapsilosis, an emerging fungal pathogen. Clin Microbiol Rev. 2008 Oct;21(4):606-25. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2570155/.
- Daneshnia F, de Almeida Júnior JN, Ilkit M, et al. Worldwide emergence of fluconazole-resistant Candida parapsilosis: current framework and future research roadmap. https://pubmed.ncbi.nlm.nih.gov/37121240/. Lancet Microbe. 2023 Jun;4(6):e470-e480.
- Fong G, et al. (2017). Candida parapsilosis Candidemia resistance patterns and treatment outcomes: An opportunity for antifungal stewardship. DOI:
https://doi.org/10.1093/ofid/ofx163.037 - Tóth R, Nosek J, Mora-Montes HM, et al. Candida parapsilosis: from Genes to the Bedsid.. https://pubmed.ncbi.nlm.nih.gov/30814115/. Clin Microbiol Rev. 2019 Feb 27;32(2):e00111-18.
- Asogan M, Kim HY, Kidd S, Alastruey-Izquierdo A, Govender NP, Dao A, Shin JH, Heim J, Ford NP, Gigante V, Sati H, Morrissey CO, Alffenaar JW, Beardsley J. Candida parapsilosis: A systematic review to inform the World Health Organization fungal priority pathogens list. Med Mycol. 2024 Jun 27;62(6):myad131. doi: 10.1093/mmy/myad131. PMID: 38935912; PMCID: PMC11210616.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


