


Last Updated on January 11, 2026 by Nurseslab.in Editorial Team
Carcinoid syndrome is a fascinating yet complex medical condition that emerges as a constellation of symptoms due to the release of certain chemicals, most notably serotonin and other vasoactive substances, into the systemic circulation by neuroendocrine tumors (NETs), more specifically carcinoid tumors.
These tumors are classified as a subset of neuroendocrine neoplasms, which predominantly arise from the enterochromaffin cells dispersed throughout the gastrointestinal tract, though they can also originate in the bronchopulmonary system and, less commonly, in other organs such as the ovaries or thymus.
Etiology and Pathophysiology
Carcinoid tumors are generally indolent, slow-growing neoplasms that are capable of synthesizing, storing, and secreting a variety of biologically active amines and peptides. The syndrome itself, however, is relatively rare and tends to manifest only when these tumors metastasize, particularly to the liver or other extraintestinal sites. Under normal physiological conditions, the portal circulation delivers the secreted substances from the gut directly to the liver, where they are metabolized and inactivated. It is only when hepatic metastases circumvent this metabolic barrier, or when the primary tumor originates outside the portal system, that these substances gain access to the systemic circulation and produce the characteristic clinical features of carcinoid syndrome.
The most prominent chemical mediators implicated in this syndrome include serotonin (5-hydroxytryptamine), histamine, bradykinins, prostaglandins, and tachykinins. Their systemic effects culminate in a unique clinical presentation that distinguishes carcinoid syndrome from other causes of neuroendocrine tumor-related symptoms.
Epidemiology
Carcinoid syndrome is considered a rare disorder. While neuroendocrine tumors have seen a rise in incidence over recent decades, owing likely to improved diagnostic methods and increased clinical awareness, only about 10% of patients with carcinoid tumors will ever develop carcinoid syndrome. Incidence rates tend to be higher in adults, typically between the ages of 50 and 70, though the syndrome can present at any age. There is no significant predilection for gender or ethnicity, and risk factors remain largely undefined, though genetic syndromes such as multiple endocrine neoplasia type 1 (MEN1) may increase susceptibility.
Clinical Features
The presentation of carcinoid syndrome can be protean, but several hallmark symptoms are recognized:
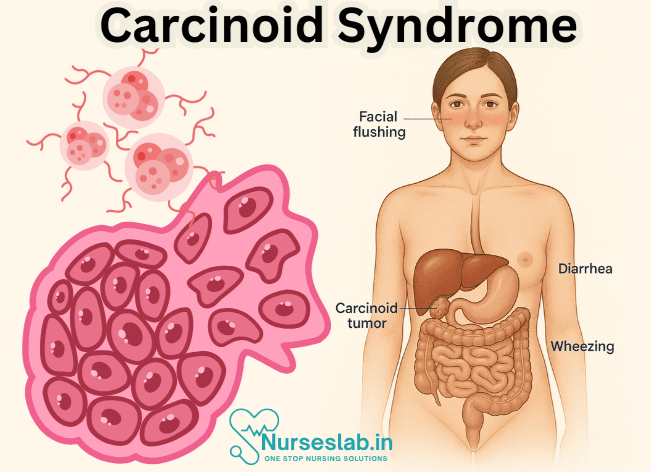
- Flushing: Perhaps the most iconic feature of carcinoid syndrome, flushing is described as a sudden, intense warmth and redness of the face, neck, and sometimes upper chest. It may last for a few minutes or extend for several hours and is often precipitated by stress, alcohol, or certain foods. Unlike the transient blush of embarrassment, this flushing tends to be more profound and is not typically associated with sweating.
- Diarrhea: Patients may experience frequent, watery, and sometimes explosive stools—often several times daily. The underlying mechanism is multifactorial, with serotonin playing a central role in stimulating intestinal secretion and motility.
- Wheezing and Bronchospasm: Up to a quarter of cases present with asthma-like symptoms, including wheezing, shortness of breath, and cough, resulting from the bronchoconstrictive properties of secreted substances.
- Cardiac Involvement: A distinctive and serious complication known as carcinoid heart disease occurs in up to 50% of patients with prolonged syndrome. Fibrotic deposits develop on the endocardial surfaces, most commonly affecting the right side of the heart (tricuspid and pulmonary valves), eventually leading to valvular dysfunction and heart failure.
- Abdominal Pain and Cramping: These symptoms may be vague and result from tumor growth, bowel obstruction, or mesenteric fibrosis.
- Niacin Deficiency: Since tryptophan is diverted toward serotonin synthesis in carcinoid tumors, the conversion to niacin (vitamin B3) is decreased, predisposing individuals to pellagra, which manifests as dermatitis, diarrhea, and dementia.
Other less common manifestations include telangiectasia, edema, and cutaneous lesions. In rare cases, patients may experience life-threatening “carcinoid crises,” characterized by profound hypotension, bronchospasm, arrhythmias, or confusion, often precipitated by anesthesia, stress, or tumor manipulation during surgery.
Diagnostic Evaluation
Diagnosing carcinoid syndrome requires a combination of clinical acumen and laboratory investigation, followed by radiological and histological confirmation.
Biochemical Markers
- 24-Hour Urinary 5-HIAA (5-hydroxyindoleacetic acid): The gold standard screening test for carcinoid syndrome. Elevated urinary 5-HIAA, a metabolite of serotonin, strongly supports the diagnosis.
- Plasma Serotonin and Chromogranin A: Measurement of these substances may provide additional information and aid in disease monitoring.
Imaging Studies
- CT and MRI: These modalities help localize the primary tumor and assess for metastatic disease.
- Somatostatin Receptor Scintigraphy (Octreoscan): Many neuroendocrine tumors express somatostatin receptors; radiolabeled octreotide scans can detect both primary and metastatic lesions with high sensitivity.
- Positron Emission Tomography (PET): Newer PET tracers such as Gallium-68-DOTATATE provide even greater sensitivity for tumor localization and staging.
Histopathology
A definitive diagnosis is achieved by biopsy of the tumor, which classically demonstrates neuroendocrine features on microscopic examination and immunohistochemical staining positive for markers such as synaptophysin and chromogranin A.
Management
Treatment of carcinoid syndrome requires a multimodal approach, focusing on symptom control, management of complications, and targeting the underlying tumor.
Symptomatic Therapy
- Somatostatin Analogs: Octreotide and lanreotide are first-line agents that inhibit secretion of serotonin and other peptides, effectively reducing flushing, diarrhea, and other symptoms.
- Antidiarrheal Agents: Loperamide and diphenoxylate-atropine may be used adjunctively.
- Serotonin Synthesis Inhibitors: Telotristat etiprate can be considered in refractory diarrhea cases, as it inhibits tryptophan hydroxylase, the rate-limiting enzyme in serotonin synthesis.
- Bronchodilators: Used as needed for bronchospasm or wheezing.
Tumor-Directed Therapy
- Surgical Resection: Where feasible, resection of the primary tumor and accessible metastases can be curative or at least palliative, reducing hormone secretion and related symptoms.
- Liver-Directed Therapies: Options include hepatic artery embolization, radiofrequency ablation, or targeted radiotherapy for patients with prominent liver metastases.
- Systemic Therapies: Peptide receptor radionuclide therapy (PRRT), interferon-alpha, and cytotoxic chemotherapy may be considered in advanced cases.
Management of Carcinoid Heart Disease
Regular echocardiographic monitoring is essential. Severe valvular dysfunction may require surgical valve replacement. Optimal control of hormone secretion is crucial to delay progression.
Prevention of Carcinoid Crisis
Patients undergoing surgery or invasive procedures must receive prophylactic high-dose octreotide to mitigate the risk of carcinoid crisis.
Prognosis
The outlook for patients with carcinoid syndrome has improved considerably with advances in diagnostic and therapeutic modalities. The five-year survival rate varies widely, dependent on the extent of disease at diagnosis and the burden of hepatic metastases. Patients with limited hepatic involvement generally fare better, while those with extensive metastases or carcinoid heart disease have a more guarded prognosis.
Living with Carcinoid Syndrome
The chronicity of symptoms can significantly impair quality of life, necessitating a multidisciplinary approach involving oncologists, cardiologists, gastroenterologists, dietitians, and mental health professionals. Patient education regarding symptom management, dietary modifications (avoiding foods high in serotonin such as bananas, walnuts, and avocados), and adherence to treatment regimens is essential.
Support groups and advocacy organizations provide invaluable resources to patients and families navigating this rare disorder.
Nursing Care of Patients with Carcinoid Syndrome
The multifaceted nature of carcinoid syndrome demands a comprehensive approach to nursing care that integrates symptom management, monitoring for complications, emotional support, education, and interprofessional collaboration.
Assessment and Nursing Diagnosis
A thorough nursing assessment should include:
- Detailed history of symptom onset, frequency, duration, and triggers (e.g., stress, alcohol, certain foods).
- Assessment of respiratory, cardiovascular, gastrointestinal, and integumentary systems.
- Monitoring for signs of complications such as heart failure, electrolyte imbalances, or malnutrition.
- Review of current medications and possible interactions.
- Evaluation of psychosocial impact, including anxiety, depression, and quality of life.
Common nursing diagnoses may include:
- Risk for impaired tissue perfusion related to recurrent flushing and vasoactive substance release.
- Risk for fluid volume deficit related to chronic diarrhea.
- Ineffective breathing pattern related to bronchospasm.
- Imbalanced nutrition, less than body requirements, related to malabsorption and increased metabolic demand.
- Anxiety related to unpredictable symptom episodes and chronic illness.
Symptom Management
Flushing
- Monitor and document frequency, duration, and severity of flushing episodes.
- Identify and educate the patient regarding potential triggers (e.g., alcohol, spicy foods, stress).
- Provide a cool, comfortable environment and encourage loose, breathable clothing.
- Administer prescribed medications (e.g., octreotide) as ordered to reduce flushing and other vasoactive symptoms.
Diarrhea
- Monitor stool frequency, consistency, and volume.
- Assess for signs and symptoms of dehydration (e.g., dry mucous membranes, decreased skin turgor, hypotension).
- Encourage increased fluid intake unless contraindicated; oral rehydration solutions may be beneficial.
- Administer antidiarrheal medications and somatostatin analogs as prescribed.
- Monitor and replace electrolytes as needed, particularly potassium, magnesium, and sodium.
- Collaborate with a dietitian to develop a nutrition plan high in protein and calories, low in triggers that worsen diarrhea.
Bronchospasm
- Monitor for signs of respiratory distress, including wheezing, tachypnea, and use of accessory muscles.
- Ensure availability and proper use of prescribed bronchodilators or corticosteroids.
- Encourage the patient to avoid known respiratory irritants (e.g., tobacco smoke, cold air).
- Position patient in semi-Fowler’s or high-Fowler’s as needed for optimal breathing.
- Provide supplemental oxygen if prescribed.
Carcinoid Heart Disease
- Monitor for symptoms of right-sided heart failure (e.g., peripheral edema, ascites, jugular venous distension).
- Assess for new or worsening cardiac murmurs and irregular heart rhythms.
- Collaborate with cardiology for ongoing evaluation and echocardiography.
- Monitor fluid balance and restrict sodium intake if indicated.
- Educate patient about symptoms of worsening heart disease and when to seek immediate care.
Pharmacologic Interventions
Nursing care involves administration and monitoring of several medications:
- Somatostatin analogs (e.g., octreotide, lanreotide): Reduce hormone secretion and control symptoms.
- Antidiarrheals: Manage persistent diarrhea.
- Bronchodilators: Relieve bronchospasm.
- Antihistamines: Mitigate effects of histamine release.
- Proton pump inhibitors or H2 blockers: Manage gastric acid hypersecretion.
- Cardiac medications: Treat carcinoid heart disease, including diuretics and digitalis if needed.
Nurses should be vigilant for medication side effects and interactions and promptly report any adverse effects to the prescribing provider.
Non-Pharmacologic Interventions and Lifestyle Modifications
- Encourage avoidance of dietary and environmental triggers (e.g., tyramine-rich foods, alcohol, stress).
- Promote a well-balanced diet tailored to the patient’s tolerance and symptoms.
- Implement energy conservation techniques to combat fatigue from chronic illness.
- Encourage scheduling of regular rest periods.
- Instruct patient and family in recognizing signs of dehydration, malnutrition, and respiratory distress.
- Advise on the importance of regular follow-up appointments for symptom monitoring and adjustment of therapies.
Monitoring and Prevention of Complications
Close monitoring and early intervention can prevent or mitigate complications:
- Frequent vital sign checks, including heart rate, respiratory rate, blood pressure, and temperature.
- Daily weights to detect fluid retention or loss.
- Lab monitoring for electrolyte imbalances, liver function, and nutritional status.
- Assessment for development or progression of cardiac disease.
- Prompt identification and management of infections, as immunosuppression is possible with certain treatments.
Psychosocial Support and Patient Education
Carcinoid syndrome often has a profound emotional and psychological impact. Nursing care should include:
- Active listening and validation of patient concerns.
- Facilitating access to mental health resources, including counseling and support groups.
- Providing education about the disease process, treatment options, and prognosis in clear, comprehensible language.
- Encouraging family involvement and offering education to caregivers on symptom management and support strategies.
Empowering patients with knowledge and coping skills can significantly improve their quality of life.
Interprofessional Collaboration
Effective management of carcinoid syndrome requires teamwork:
- Coordinate with physicians, pharmacists, dietitians, social workers, and mental health professionals.
- Participate in interdisciplinary case conferences for complex cases.
- Ensure clear, timely communication about changes in patient status and treatment plans.
Patient Safety Considerations
- Implement fall precautions for patients with weakness or dizziness.
- Monitor for signs of acute carcinoid crisis—a potentially life-threatening complication characterized by profound flushing, hypotension, bronchospasm, and arrhythmias. Have emergency protocols in place and educate the patient on when to seek immediate care.
- Encourage medication adherence and safe administration, providing reminders and organizational tools if needed.
Discharge Planning and Community Resources
Planning for ongoing care after hospitalization or diagnosis is crucial:
- Arrange for home health nursing if needed for medication administration or monitoring.
- Provide information on community resources, such as local or online support groups for patients with neuroendocrine tumors.
- Educate about the importance of adherence to follow-up appointments for ongoing evaluation and treatment adjustment.
REFERENCES
- Clement D, Ramage J, Srirajaskanthan R. Update on Pathophysiology, Treatment, and Complications of Carcinoid Syndrome.. https://pubmed.ncbi.nlm.nih.gov/32322270/J Oncol. 2020 Jan 21;2020:8341426.
- Ferri FF. Carcinoid syndrome. In: Ferri’s Clinical Advisor 2021. Elsevier; 2021. https://www.clinicalkey.com
- Feldman M, et al. Neuroendocrine tumors. In: Sleisenger and Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology, Diagnosis, Management. 11th ed. Elsevier; 2021. https://www.clinicalkey.com.
- Koumarianou A, Daskalakis K, Tsoli M, Kaltsas G, Pavel M. Efficacy, safety and unmet needs of evolving medical treatments for carcinoid syndrome.. https://pubmed.ncbi.nlm.nih.gov/35794780/ J Neuroendocrinol. 2022 Jul;34(7):e13174.
- Menon G, Pandit S, Annamaraju P, et al. Carcinoid Syndrome. [Updated 2025 Feb 18]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/sites/books/NBK448096/
- Maxwell JE, Naraev B, Halperin DM, Choti MA, Halfdanarson TR. Shifting Paradigms in the Pathophysiology and Treatment of Carcinoid Crisis. https://pubmed.ncbi.nlm.nih.gov/35165817/. Ann Surg Oncol. 2022 May;29(5):3072-3084.
- Wolin EM, Benson Iii AB. Systemic Treatment Options for Carcinoid Syndrome: A Systematic Review.. https://pubmed.ncbi.nlm.nih.gov/31018209/ Oncology. 2019;96(6):273-289.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


