


Last Updated on January 8, 2026 by Nurseslab.in Editorial Team
Cerebellar degeneration involves the gradual loss of neurons in the cerebellum, affecting movement, speech, and eye control. Causes include genetic mutations, alcohol abuse, autoimmune disorders, and cancer. Treatment focuses on symptom relief and supportive care.
Introduction
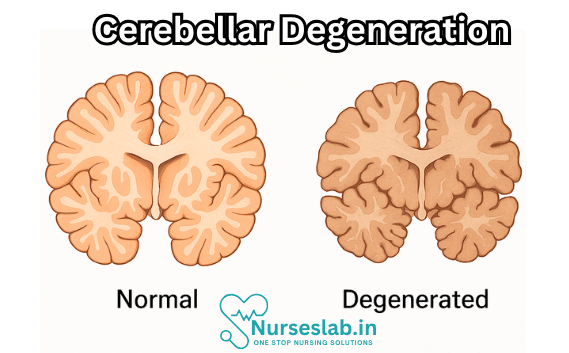
Cerebellar Degeneration Disease (CDD) represents a group of neurological disorders characterised by the progressive loss of cells in the cerebellum, a vital part of the brain responsible for coordinating movement, maintaining balance, and regulating certain cognitive functions. The impact of cerebellar degeneration is profound, affecting the quality of life, independence, and wellbeing of patients.
Pathophysiology of Cerebellar Degeneration
Cerebellar degeneration involves the gradual loss or dysfunction of neurons within the cerebellum, particularly the Purkinje cells, which are crucial for cerebellar output. The pathophysiological processes vary depending on the underlying cause but often include:
- Neuronal Death: Programmed cell death (apoptosis) or necrosis of cerebellar neurons, especially Purkinje cells and granule cells.
- Demyelination: Loss of the myelin sheath surrounding nerve fibres, disrupting signal transmission.
- Glial Activation: Reactive changes in glial cells, which can contribute to inflammation and further neuronal injury.
- Accumulation of Toxic Proteins: In some genetic forms, abnormal proteins accumulate within neurons, leading to dysfunction and cell death.
At the molecular level, oxidative stress, mitochondrial dysfunction, and impaired cellular signalling are common features contributing to disease progression. The interplay of genetic, environmental, and immunological factors determines the specific mechanisms in individual cases.
Causes and Risk Factors
Cerebellar degeneration can arise from a range of causes, broadly categorised into genetic, acquired, and idiopathic forms.
Genetic Causes
- Spinocerebellar Ataxias (SCAs): A group of inherited disorders, often autosomal dominant, characterised by progressive cerebellar atrophy and ataxia.
- Friedreich’s Ataxia: An autosomal recessive disorder affecting both the cerebellum and spinal cord, often presenting in childhood or adolescence.
- Other Hereditary Ataxias: Includes episodic ataxias, ataxia-telangiectasia, and mitochondrial disorders.
Acquired Causes
- Alcohol Abuse: Chronic excessive alcohol intake is a leading cause of acquired cerebellar degeneration, often termed alcoholic cerebellar degeneration.
- Paraneoplastic Syndromes: Immune-mediated degeneration associated with underlying malignancies, particularly small-cell lung cancer and gynaecological tumours.
- Vitamin Deficiencies: Deficiency of vitamin E or thiamine (vitamin B1) can lead to cerebellar dysfunction.
- Infections: Certain viral or bacterial infections can trigger immune-mediated cerebellar injury.
- Toxins and Medications: Exposure to heavy metals (e.g., mercury, lead), anti-epileptic drugs, or chemotherapy agents can be contributory.
- Autoimmune Disorders: Conditions such as gluten ataxia or multiple sclerosis may involve immune attack on cerebellar tissue.
Idiopathic Forms
In some cases, no clear cause can be identified despite thorough investigation. These are termed idiopathic cerebellar ataxias and may have a variable clinical course.
Risk Factors
- Family history of hereditary ataxias
- Chronic alcohol consumption
- History of cancer (risk of paraneoplastic syndromes)
- Malnutrition or poor dietary intake
- Exposure to neurotoxic substances
- Autoimmune predisposition
Clinical Manifestations
The hallmark of cerebellar degeneration is ataxia, a condition characterised by unsteady gait, poor coordination, and difficulties with fine motor tasks. However, the clinical spectrum extends beyond motor symptoms.
Motor Symptoms
- Gait Ataxia: Broad-based, unsteady walking pattern; frequent stumbling or falls.
- Limb Ataxia: Clumsiness, intention tremor, difficulty with tasks requiring precise hand movements.
- Dysarthria: Slurred, slow, or scanning speech due to impaired muscle coordination.
- Dysmetria: Inability to judge distance or scale movements appropriately.
- Nystagmus: Involuntary, rapid eye movements that may impair vision.
- Hypotonia: Reduced muscle tone, leading to floppy limb appearance.
Non-Motor Symptoms
- Cognitive Impairments: Difficulties with planning, attention, or executive function.
- Emotional Changes: Mood swings, depression, or irritability.
- Autonomic Dysfunction: Problems with bladder control, blood pressure, or heart rate (less common).
- Oculomotor Abnormalities: Difficulty in controlling eye movements, leading to double vision or visual tracking issues.
Progression
The rate of progression varies depending on the underlying cause. Hereditary forms often progress slowly over years or decades, while paraneoplastic and some acquired forms may advance rapidly.
Diagnosis
Diagnosing cerebellar degeneration requires a comprehensive clinical evaluation, supported by neuroimaging and laboratory investigations. The diagnostic process aims to identify the underlying cause, assess the extent of cerebellar involvement, and rule out other conditions that may mimic ataxia.
Clinical Evaluation
- Detailed medical and family history, including onset and progression of symptoms.
- Neurological examination focusing on gait, coordination, speech, and eye movements.
Imaging Studies
- Magnetic Resonance Imaging (MRI): The gold standard for visualising cerebellar atrophy, identifying structural lesions, and excluding other pathologies.
- Computed Tomography (CT): May reveal cerebellar shrinkage but is less sensitive than MRI.
Laboratory Tests
- Blood tests for vitamin deficiencies, autoimmune markers, and metabolic screening.
- Genetic testing for hereditary ataxias, particularly if there is a family history or early onset.
- Paraneoplastic antibody panels in cases with suspected malignancy-associated ataxia.
- Cerebrospinal fluid analysis if infection or inflammation is suspected.
Differential Diagnosis
- Multiple sclerosis
- Stroke or transient ischaemic attack
- Brain tumours
- Peripheral neuropathy
- Vestibular disorders
- Psychogenic movement disorders
A multidisciplinary approach involving neurologists, geneticists, and rehabilitation specialists is often essential for accurate diagnosis and management planning.
Treatment Options
Currently, there is no cure for most forms of cerebellar degeneration. Treatment is primarily supportive, aiming to alleviate symptoms, slow progression, and improve quality of life. Management strategies vary depending on the underlying cause and individual patient needs.
Pharmacological Treatments
- Immunotherapy: In paraneoplastic and autoimmune ataxias, immunosuppressive therapies (e.g., corticosteroids, intravenous immunoglobulin, plasma exchange) may be beneficial.
- Vitamin Supplementation: Correction of vitamin E or thiamine deficiency can halt or reverse symptoms in deficiency-related ataxias.
- Symptomatic Medications: Drugs to manage tremor, spasticity, or mood disturbances (e.g., propranolol, baclofen, antidepressants).
Rehabilitative Therapies
- Physiotherapy: Exercises to maintain mobility, balance, and muscle strength; gait training and fall prevention strategies.
- Occupational Therapy: Techniques and assistive devices to promote independence in daily activities.
- Speech and Language Therapy: Support for dysarthria and swallowing difficulties.
Surgical and Advanced Therapies
- Deep Brain Stimulation: Experimental in cerebellar ataxias; may benefit selected patients with severe tremor.
- Stem Cell Therapy: Under investigation; not yet established as standard care.
Supportive Care
- Education and counselling for patients and families
- Psychological support for coping with chronic illness
- Management of complications such as falls, aspiration, or pressure sores
- Social services and community resources for disability support
Prognosis and Complications
The prognosis of cerebellar degeneration varies widely. In hereditary forms, such as spinocerebellar ataxias, the disease often progresses slowly but leads to increasing disability over time. Life expectancy may be reduced in certain types, especially when accompanied by cardiac or respiratory involvement (e.g., Friedreich’s ataxia).
Potential complications include falls and fractures, aspiration pneumonia due to swallowing difficulties, malnutrition, depression, and social isolation. Early intervention and multidisciplinary care can mitigate some of these risks and help maintain the best possible quality of life.
Living with Cerebellar Degeneration
A diagnosis of cerebellar degeneration brings significant physical, emotional, and practical challenges. Comprehensive support is essential for both patients and caregivers.
Patient Support Resources
- Patient Advocacy Groups: Organisations such as Ataxia UK, National Ataxia Foundation (USA), and Indian organisations like Ataxia Awareness India provide information, support, and advocacy.
- Rehabilitation Services: Access to physiotherapists, occupational therapists, and speech therapists is vital for maximising independence.
- Counselling and Mental Health Support: Addressing anxiety, depression, and adjustment issues is integral to holistic care.
- Peer Support Networks: Connecting with others living with ataxia can reduce isolation and share coping strategies.
- Assistive Devices: Use of walking aids, adaptive utensils, and communication tools can improve safety and autonomy.
- Legal and Financial Advice: Guidance on disability rights, insurance, and benefits is often necessary.
Nursing Care of Patients with Cerebellar Degeneration
Cerebellar degeneration is a progressive neurological disorder characterized by the loss of neurons in the cerebellum, the area of the brain responsible for coordination, balance, and fine motor control. Patients with cerebellar degeneration present with a range of symptoms, including ataxia, dysarthria, nystagmus, tremors, and difficulties with gait and coordination. The underlying causes can vary from genetic conditions such as spinocerebellar ataxia to acquired causes like chronic alcohol use, vitamin deficiencies, paraneoplastic syndromes, or autoimmune conditions.
Due to the multifaceted impact of cerebellar degeneration on a patient’s physical, psychological, and social well-being, nursing care requires a holistic, patient-centered approach.
1. Assessment
Effective nursing care begins with a thorough assessment, which includes:
- Neurological status: Assess for changes in gait, balance, coordination, muscle tone, and reflexes. Note the presence of intention tremors, dysdiadochokinesia (difficulty with rapid alternating movements), and dysmetria (improper judging of distances).
- Speech and swallowing: Observe for dysarthria (slurred speech) and dysphagia, as these are common and may increase the risk of aspiration.
- Vision and eye movement: Monitor for nystagmus and other visual disturbances.
- Cognitive and psychological status: Evaluate mood, cognitive functioning, and coping mechanisms, as chronic neurological diseases can lead to depression and anxiety.
- Activities of daily living (ADLs): Assess the patient’s ability to perform self-care, including feeding, dressing, bathing, and toileting.
- Fall risk: Identify environmental hazards and evaluate the need for assistive devices.
2. Nursing Diagnoses
Common nursing diagnoses for patients with cerebellar degeneration may include:
- Impaired physical mobility related to muscular incoordination and ataxia
- Risk for injury related to balance disturbances and falls
- Impaired verbal communication related to dysarthria
- Impaired swallowing (dysphagia) with risk of aspiration
- Self-care deficit related to incoordination and tremor
- Disturbed body image and risk for social isolation
- Risk for depression and altered coping mechanisms
3. Planning and Goal Setting
The primary goals in the care of patients with cerebellar degeneration are to:
- Promote safety and prevent falls or injuries
- Maintain maximum independence in ADLs
- Improve communication and swallowing functions
- Support psychological well-being
- Educate patients and caregivers about disease management
Each care plan should be individualized based on the patient’s specific symptoms, progression of the disease, and support system.
4. Implementation of Nursing Interventions
4.1 Promoting Safety and Preventing Injury
- Environmental modification: Remove clutter, secure loose rugs, and install grab bars in bathrooms and hallways. Ensure adequate lighting, especially at night.
- Use of assistive devices: Recommend canes, walkers, wheelchairs, or orthotic devices as appropriate. Refer to physical therapy for gait training and balance exercises.
- Supervision: Supervise at-risk patients during transfers and ambulation. Educate caregivers about safe transfer techniques.
- Bed safety: Keep the bed at a low height and use padded side rails if needed to prevent falls.
4.2 Supporting Mobility and Independence
- Physical therapy: Collaborate with physical therapists for range-of-motion exercises, strengthening, and balance training to optimize mobility.
- Occupational therapy: Facilitate adaptive techniques and use of specialized utensils for eating, dressing aids, and other equipment to promote independence.
- Energy conservation: Encourage rest periods and teach patients to pace activities to prevent fatigue.
4.3 Managing Communication and Swallowing Difficulties
- Speech therapy: Refer for speech therapy to improve articulation and develop alternative communication strategies as needed (e.g., communication boards, electronic devices).
- Swallowing assessment: Coordinate with speech-language pathologists to assess dysphagia and recommend appropriate dietary modifications (e.g., thickened liquids, pureed foods).
- Safe feeding: Position the patient upright during meals and advise slow, deliberate chewing and swallowing. Monitor closely for signs of aspiration such as coughing, choking, or wet voice.
4.4 Facilitating Self-Care
- Adaptive equipment: Provide tools such as non-slip mats, weighted utensils, and grab bars to aid in self-care tasks.
- Structuring routines: Establish predictable routines to reduce stress and confusion.
- Encouragement: Offer positive reinforcement and encouragement to foster independence, even if tasks take longer to complete.
4.5 Addressing Psychosocial and Emotional Needs
- Therapeutic communication: Listen actively and validate feelings of frustration, fear, or loss.
- Support groups: Encourage participation in support groups for individuals with similar conditions and their families.
- Mental health referrals: Refer to counseling or psychiatric services if depression, anxiety, or adjustment disorders are suspected.
- Education: Teach patients and families about the disease process, progression, and expectations to empower decision-making and coping.
4.6 Monitoring and Managing Medical Complications
- Medication management: Administer prescribed medications, which may include muscle relaxants, antispasmodics, or drugs for associated symptoms such as spasticity or tremor. Monitor for side effects and drug interactions.
- Nutritional support: Track weight, hydration status, and nutritional intake. Collaborate with dietitians as needed to ensure proper nutrition and address swallowing difficulties.
- Preventing secondary complications: Implement interventions to prevent pressure ulcers, urinary tract infections, and respiratory complications due to immobility or aspiration.
5. Evaluation
Regularly reassess the patient’s status and the effectiveness of interventions. Modify the care plan as the disease progresses or new needs arise. Evaluation should include:
- Patient’s ability to perform ADLs and level of independence
- Frequency of falls or injuries
- Effectiveness of communication and swallowing interventions
- Psychological adjustment and support system adequacy
6. Patient and Caregiver Education
Education is an ongoing process and is critical for empowering patients and caregivers:
- Teach about the nature of cerebellar degeneration, expected symptoms, and progression
- Demonstrate safe use of adaptive equipment and transfer techniques
- Provide written instructions and resources for community support services
- Encourage advance care planning and discussion of wishes regarding future care
7. Multidisciplinary Collaboration
Optimal care requires collaboration among healthcare professionals, including:
- Neurologists for ongoing evaluation and disease management
- Physical, occupational, and speech therapists for rehabilitation
- Dietitians for nutritional assessment and intervention
- Social workers for community resource coordination and psychosocial support
- Mental health professionals for counseling and psychiatric care
8. End-of-Life Considerations
In advanced stages, cerebellar degeneration can severely limit independence and quality of life. Nurses play a key role in:
- Providing comfort care and symptom management
- Supporting families through anticipatory grief and decision-making
- Facilitating hospice or palliative care referrals as appropriate
REFERENCES
- Ataullah AHM, Naqvi IA. Cerebellar Dysfunction. https://www.ncbi.nlm.nih.gov/books/NBK562317/. [Updated 2021 July 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-.
- National Center for Advancing Translational Sciences. Genetic and Rare Diseases (GARD) Information Center. Cerebellar degeneratio.. https://rarediseases.info.nih.gov/diseases/6019/cerebellar-degeneration.
- National Organization for Rare Disorders (NORD). Subacute Cerebellar Degeneration. https://rarediseases.org/rare-diseases/cerebellar-degeneration-subacute/.
- Liu G, Yang C, Wang X, Chen X, Cai H, Le W. Cerebellum in neurodegenerative diseases: Advances, challenges, and prospects. iScience. 2024 Oct 18;27(11):111194. doi: 10.1016/j.isci.2024.111194. PMID: 39555407; PMCID: PMC11567929.
- Ilg W, Bastian AJ, Boesch S, Burciu RG, Celnik P, Consensus paper: management of degenerative cerebellar disorders. Cerebellum. 2014 Apr;13(2):248-68.
- Akanksha Sharma, 15 Warning Signs of Cerebellar Degeneration, https://healthprep.com/slideshow/conditions/15-warning-signs-of-cerebellar-degeneration/
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


