


Last Updated on January 21, 2026 by Nurseslab.in Editorial Team
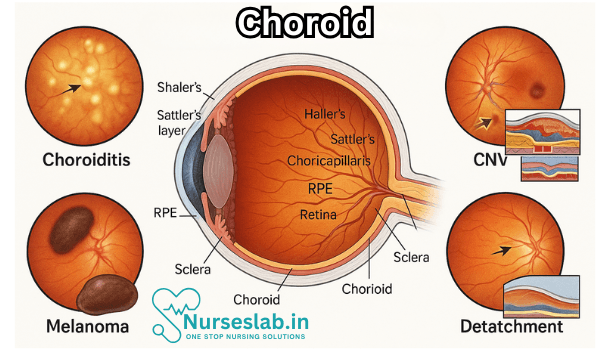
Explore the Choroid Diseases : a vascular tissue layer that lies between the sclera and retina. It plays a crucial role in nourishing retinal cells, maintaining temperature balance, and supporting photoreceptor function. Understanding the choroid is essential in diagnosing and managing eye conditions such as choroiditis, macular degeneration, and other retinal disorders.
Introduction
The human eye is a highly specialised organ, comprising multiple layers and structures that work in harmony to facilitate vision. Among these layers, the choroid is a critical yet often overlooked component. Situated between the retina and the sclera, the choroid is a vascular layer that plays a pivotal role in nourishing the outer retina, maintaining ocular temperature, and regulating intraocular pressure. Diseases of the choroid, collectively referred to as choroidopathies or choroid diseases, can lead to significant visual impairment or even blindness if not diagnosed and managed promptly.
Types of Choroid Diseases
Choroid diseases encompass a wide spectrum of conditions, ranging from inflammatory and degenerative disorders to neoplastic and vascular pathologies. Some of the most common and clinically significant choroid diseases are discussed below.
1. Choroiditis
Choroiditis refers to inflammation of the choroid and can be classified as infectious or non-infectious.
Infectious Choroiditis:
- Tuberculous Choroiditis: Tuberculosis (TB) remains endemic in India, and ocular TB can manifest as choroiditis. Patients may present with multifocal choroidal lesions, serous retinal detachment, or choroidal granulomas. Diagnosis often relies on a combination of clinical suspicion, imaging, and laboratory tests (e.g., Mantoux test, interferon-gamma release assays).
- Toxoplasma Choroiditis: Caused by the protozoan Toxoplasma gondii, this form is characterised by focal necrotising retinochoroiditis, commonly known as “headlight in the fog” appearance due to active lesions surrounded by vitreous haze.
- Other Infections: Syphilis, cytomegalovirus, herpes viruses, and fungal agents can also infect the choroid, especially in immunocompromised individuals.
Non-Infectious Choroiditis:
Vogt-Koyanagi-Harada (VKH) Disease: An autoimmune disorder targeting melanocyte-containing tissues, VKH presents with bilateral granulomatous panuveitis, serous retinal detachments, and systemic features like poliosis, vitiligo, and meningism.
Birdshot Chorioretinopathy: Characterised by multiple cream-coloured choroidal spots and strong association with HLA-A29 antigen, mostly seen in middle-aged adults.
2. Choroidal Neovascularisation (CNV)
Choroidal neovascularisation involves the growth of abnormal blood vessels from the choroid into the subretinal space. This process is central to several sight-threatening conditions, most notably:
- Age-Related Macular Degeneration (AMD): The most common cause of CNV in older adults, especially in developed countries, but increasingly recognised in urban Indian populations due to rising life expectancy.
- High Myopia: Pathological myopia can cause degenerative changes leading to CNV, particularly in younger adults.
- Ocular Histoplasmosis and Angioid Streaks: Both can predispose to the development of CNV.
Clinically, CNV presents with sudden onset of visual distortion (metamorphopsia), central scotoma, and decreased visual acuity. Fluorescein angiography and optical coherence tomography (OCT) are essential diagnostic tools.
3. Choroidal Tumours
The choroid is the most common site for intraocular tumours in adults.
- Choroidal Melanoma: The most prevalent primary intraocular malignancy in adults, though rarer in Indian populations compared to Caucasians. Presents as a pigmented or non-pigmented mass, often detected incidentally or due to visual symptoms.
- Choroidal Haemangioma: Benign vascular tumours that may cause visual impairment due to exudative retinal detachment.
- Metastatic Tumours: Commonly originate from breast or lung primaries and may present as creamy, yellowish choroidal lesions.
4. Central Serous Chorioretinopathy (CSCR)
CSCR is a condition characterised by serous detachment of the neurosensory retina, often due to leakage of fluid through the retinal pigment epithelium (RPE) from the choroid. It primarily affects young and middle-aged adults, with a higher prevalence among Indian males. Stress, corticosteroid use, and type A personality have been implicated as risk factors. Patients present with blurred vision, micropsia, and metamorphopsia. OCT and fluorescein angiography are crucial for diagnosis.
5. Choroidal Dystrophies
These are inherited degenerative conditions affecting the choroid, often leading to progressive vision loss.
- Gyrate Atrophy: An autosomal recessive disorder resulting in sharply demarcated areas of chorioretinal atrophy, often detected in childhood or adolescence.
- Choroideremia: An X-linked recessive disease leading to progressive degeneration of the choroid, RPE, and retina, with night blindness as an early symptom.
- Central Areolar Choroidal Dystrophy: Presents in adulthood with central vision loss due to atrophy of the macular choroid.
6. Choroidal Detachment
Choroidal detachment occurs when fluid or blood accumulates in the suprachoroidal space, separating the choroid from the sclera. Common causes include ocular trauma, postoperative complications, hypotony, and inflammation. Symptoms include pain, decreased vision, and a shallow anterior chamber. B-scan ultrasonography is often employed for diagnosis.
Pathogenesis and Risk Factors
The aetiology of choroid diseases is multifactorial and depends on the specific condition. Some common risk factors include:
- Genetic predisposition (e.g., choroidal dystrophies, AMD)
- Infections (e.g., TB, toxoplasmosis)
- Autoimmune mechanisms (e.g., VKH disease)
- Environmental factors (e.g., stress in CSCR)
- Systemic diseases (e.g., diabetes, hypertension)
- Ageing (e.g., AMD)
- Lifestyle factors (e.g., smoking, corticosteroid use)
Understanding these risk factors is crucial for both prevention and early intervention.
Clinical Presentation
The clinical features of choroid diseases are variable and depend on the underlying pathology. Common symptoms include:
- Blurred or distorted vision
- Scotomas (blind spots)
- Photopsia (flashes of light)
- Metamorphopsia (distorted images)
- Decreased night vision
- Visual field defects
- Ocular pain (in inflammatory or traumatic conditions)
On examination, findings may include choroidal lesions, serous or haemorrhagic detachments, neovascular membranes, or masses.
Diagnostic Approaches
Accurate diagnosis of choroid diseases often requires a combination of clinical evaluation and advanced imaging techniques:
- Fundus Examination: Direct and indirect ophthalmoscopy to visualise choroidal changes.
- Optical Coherence Tomography (OCT): Provides high-resolution cross-sectional images of the retina and choroid, essential for detecting subretinal fluid, CNV, and structural changes.
- Fluorescein Angiography (FA): Useful for visualising retinal and choroidal vasculature, leakage, and neovascular membranes.
- Indocyanine Green Angiography (ICGA): Superior for visualising choroidal vasculature, especially in diseases like polypoidal choroidal vasculopathy.
- B-Scan Ultrasonography: Helpful in detecting choroidal tumours, detachments, and posterior segment pathologies when media opacities exist.
- Laboratory Tests: Including serology for infections, autoimmune markers, and genetic testing for inherited conditions.
The choice of investigations depends on the suspected diagnosis and available resources.
Management Strategies
Treatment of choroid diseases is highly individualised and depends on the specific condition, severity, and underlying cause.
1. Medical Management
- Anti-inflammatory Therapy: Corticosteroids (topical, periocular, systemic) are the mainstay for non-infectious choroiditis, with immunosuppressive agents (e.g., azathioprine, cyclosporine) used for refractory cases.
- Antimicrobial Therapy: Appropriate antibiotics or antiparasitic agents for infectious choroiditis (e.g., anti-TB therapy, anti-toxoplasma drugs).
- Anti-VEGF Therapy: Intravitreal injections of anti-vascular endothelial growth factor agents (e.g., ranibizumab, aflibercept) are the standard of care for CNV secondary to AMD, myopia, or other causes.
- Observation: In self-limiting conditions like acute CSCR, observation and risk factor modification may suffice.
2. Surgical and Laser Interventions
- Photodynamic Therapy (PDT): Used for chronic CSCR and some types of CNV.
- Laser Photocoagulation: Focal or grid laser for extrafoveal CNV or leaking points in CSCR.
- Vitrectomy: Indicated for complications like vitreous haemorrhage, retinal detachment, or non-resolving CNV.
- Enucleation: Rarely, removal of the eye may be necessary for large malignant tumours.
3. Supportive and Rehabilitation Measures
- Low Vision Aids: Optical and electronic devices to maximise residual vision in cases of irreversible visual loss.
- Counselling: Psychological support and vocational rehabilitation for patients with significant vision impairment.
- Regular Monitoring: Essential for early detection of disease recurrence or complications.
Prognosis
The prognosis of choroid diseases varies widely depending on the specific condition, timely diagnosis, and adequacy of treatment. Conditions like acute CSCR may resolve spontaneously with good visual recovery, while diseases like choroidal melanoma or advanced CNV can result in permanent vision loss if untreated. Early intervention, patient education, and regular follow-up are key to optimising outcomes.
Prevention and Public Health Considerations
Many choroid diseases, especially those with infectious aetiologies, can be prevented through public health measures such as:
- Effective control of systemic infections (e.g., TB control programmes)
- Health education regarding safe food and water practices to prevent toxoplasmosis
- Encouraging regular eye check-ups, especially in high-risk groups (elderly, diabetics, highly myopic individuals)
- Promoting healthy lifestyle practices to reduce stress and limit corticosteroid use
- Genetic counselling for families with inherited choroidal dystrophies
In India, increasing awareness about ocular health and access to specialised eye care services remain critical challenges.
Nursing Care of Patients with Choroidal Disorders
Effective nursing care of patients with choroidal disorders is essential for promoting healing, preventing complications, and supporting psychosocial wellbeing.
Assessment and Diagnosis
The first step in nursing care is a comprehensive assessment, which includes:
- Detailed health history, focusing on ocular symptoms (blurred vision, photophobia, pain, floaters).
- Observation for redness, swelling, or discharge in the affected eye.
- Assessment of visual acuity and visual fields.
- Monitoring for systemic symptoms such as fever, malaise, or headache if infection is suspected.
- Review of diagnostic procedures (fundoscopy, optical coherence tomography, ultrasonography, fluorescein angiography), as prescribed by the physician.
Planning Nursing Care
Nursing care for patients with choroidal disorders should be individualized, evidence-based, and holistic. Key goals include:
- Relieving ocular discomfort and pain.
- Preventing further damage to ocular structures.
- Maintaining or improving visual function.
- Supporting psychological and emotional wellbeing.
- Educating patients and families about the disorder, management, and prevention of complications.
Interventions in Nursing Care
Pain and Symptom Management
- Administer prescribed medications: Analgesics, anti-inflammatory drugs, corticosteroids, immunosuppressives, or antibiotics as indicated by the underlying cause.
- Monitor for adverse effects: Regularly assess for side effects of eye medications, particularly steroids and immunosuppressants.
- Apply cold compresses: May help reduce local inflammation and discomfort.
- Provide a calm environment: Minimize light exposure and limit screen time; suggest use of sunglasses for photophobia.
Monitoring and Prevention of Complications
- Monitor visual changes: Document changes in vision, emergence of new symptoms, and report promptly to the physician.
- Observe for signs of increased intraocular pressure: Headache, nausea, vomiting, sudden vision loss—may indicate risk of glaucoma.
- Prevent infection: Teach proper hand hygiene, avoid touching or rubbing the eyes, and maintain sterile technique during medication administration.
- Support wound healing: For postsurgical or post-traumatic cases, monitor surgical sites for infection, bleeding, or discharge.
- Assist with eye protection: Advise use of eye shields or protective glasses as needed.
Psychosocial Support
- Address anxiety and fear: Provide empathetic communication, allow expression of feelings and concerns about vision loss or diagnosis.
- Support coping strategies: Recommend support groups or counseling where appropriate.
- Facilitate independence: Encourage participation in self-care, provide orientation for patients with reduced vision, and offer environmental modifications to enhance safety.
Patient and Family Education
- Teach disease process: Explain the nature of the choroidal disorder, expected symptoms, and prognosis in accessible terms.
- Explain medication regimen: Review purpose, proper administration, potential side effects, and the importance of adherence.
- Discuss warning signs: Instruct patients to promptly report any sudden changes in vision, severe eye pain, or new symptoms.
- Promote regular follow-up: Encourage routine ophthalmologic checkups for early detection of complications.
- Advise on lifestyle modifications: Limit activities that may strain the eyes, advise a healthy diet rich in antioxidants, and recommend smoking cessation if applicable.
Special Considerations for Specific Choroidal Conditions
Choroiditis
- Monitor for systemic involvement (e.g., in cases of infectious or autoimmune causes).
- Administer prescribed anti-infectives or immunomodulatory therapy.
- Coordinate with multidisciplinary team (infectious disease, rheumatology) as needed.
Choroidal Melanoma
- Provide pre- and post-operative care for patients undergoing surgical intervention, radiation, or laser therapy.
- Monitor for signs of tumor progression or metastasis.
- Offer emotional support in coping with cancer diagnosis and treatment.
Choroidal Detachment
- Assist in emergency management if vision is acutely compromised.
- Prepare patient for possible surgical repair or drainage procedures.
- Monitor fluid balance and systemic status if detachment is secondary to trauma or severe inflammation.
Documentation and Communication
Accurate, timely documentation is critical in the nursing management of choroidal disorders. Record all assessments, interventions, patient responses, and communications with the healthcare team. Ensure that any changes in condition are reported promptly to facilitate early intervention.
Discharge Planning and Home Care
Upon discharge, patients require clear instructions and support for ongoing self-care:
- Medication management: Confirm understanding of dosing, administration, and medication storage.
- Signs and symptoms to report: Reinforce education on complications or emergencies.
- Follow-up care: Schedule appointments with ophthalmology and other specialties as required.
- Vision rehabilitation: Refer to low-vision services for adaptive equipment and training.
REFERENCES
- Ehrlich R, Harris A, Wentz SM, Moore NA, Siesky BA. Anatomy of the Optic Nerve Blood Flow. Reference Module in Neuroscience and Biobehavioral Psychology. Elsevier. 2017.
- Evans R. Anatomy of the Uvea. In: Vanoff M and Duker JS, eds. Ophthalmology. 6th ed. Elsevier. 2023:631-633.
- Barth T, Helbig H. Ischemic Choroidal Diseases. Klin Monbl Augenheilkd. 2021 Sep;238(9):962-970. English, German. doi: 10.1055/a-1402-7592. Epub 2021 Aug 20. PMID: 34416787.
- Regatieri CVS. Retinal and Choroidal Circulation. In: Vanoff M and Duker JS (eds), Ophthalmology. 6th ed. Elsevier. 2023:399-403.
- Rehman I, Hazhirkarzar B, Patel BC. Anatomy, Head and Neck, Eye. https://www.ncbi.nlm.nih.gov/books/NBK482428/. 2023 Jul 24. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan. Accessed 11/4/2024.
- Riordan-Eva P. Anatomy & Embryology of the Eye. In: Riordan-Eva P, Augsburger JJ, eds. Vaughan & Asbury’s General Ophthalmology. 19th ed. McGraw-Hill Education; 2017.
- Samuels B. Ocular Disorders. In: Amthor FR, Theibert AB, Standaert DG, Roberson ED, eds. Essentials of Modern Neuroscience. McGraw Hill; 2020.
- Chua J, Tan B, Wong D, Garhöfer G, Liew XW, Popa-Cherecheanu A, Loong Chin CW, Milea D, Li-Hsian Chen C, Schmetterer L. Optical coherence tomography angiography of the retina and choroid in systemic diseases. Prog Retin Eye Res. 2024 Nov;103:101292. https://pubmed.ncbi.nlm.nih.gov/39218142/
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


