


Last Updated on January 12, 2026 by Nurseslab.in Editorial Team
Josephine Paterson and Loretta Zderad’s Humanistic Nursing Theory is a profound and experiential framework that centers on the lived relationship between nurse and patient. It’s grounded in existentialism and phenomenology, emphasizing the uniqueness of each human encounter and the mutual growth that can occur through authentic dialogue.
Life Story of Josephine Paterson
Josephine Paterson (born September 1, 1924, in Freeport, New York) was a visionary nurse theorist who, alongside Loretta Zderad, developed the Humanistic Nursing Theory a groundbreaking framework that emphasizes the lived experience, dialogue, and mutual growth between nurse and patient.

Early Life & Education
- Graduated from Lenox Hill School of Nursing in August 1945.
- Earned her Master’s degree from Johns Hopkins School of Hygiene and Public Health in 1954.
- Completed her Doctorate in Nursing at Boston University, specializing in psychiatric nursing.
Career & Collaboration
- Met Loretta Zderad in the 1950s while both were employed at Catholic University.
- Paterson worked as a psychotherapist at the Mental Hygiene Clinic; Zderad was promoted to Associate Chief of Nursing Service for Education.
- Their friendship and professional partnership spanned over 35 years, culminating in the development of their theory.
- Retired in 1985 as a Clinical Nurse Specialist at Northport Veterans Administration Medical Center, New York.
Humanistic Nursing Theory
Published in Humanistic Nursing (1976), the theory is rooted in existentialism and phenomenology, focusing on:
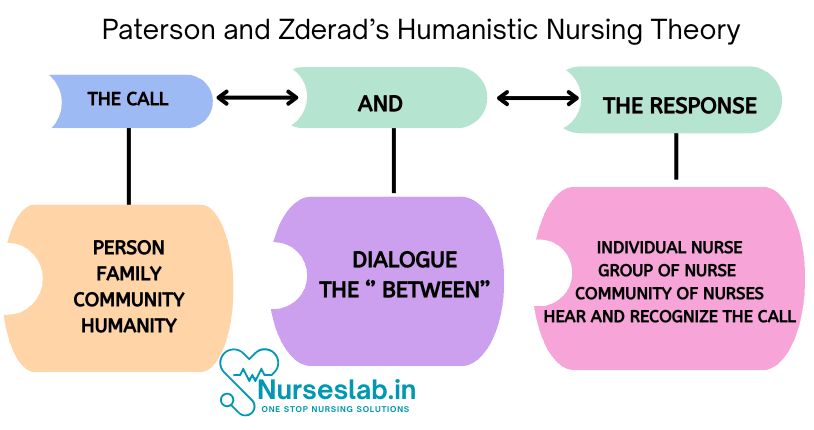
- Dialogue: A reciprocal, authentic exchange between nurse and patient.
- Presence: The nurse’s openness, receptivity, and availability.
- Call and Response: The nurse hears and responds to the patient’s call for help.
- Five Phases of Inquiry:
- Preparing the nurse knower for coming to know
- Intuitive knowing of the other
- Scientific knowing of the other
- Complementary synthesis
- Succession from many to paradoxical one
The theory encourages nurses to reflect on their own experiences and values, fostering self-actualization and more being helping patients become more humanly possible in their unique life situations.
Legacy
- Paterson’s work continues to influence nursing education, palliative care, and holistic practice.
- Her theory is widely taught and applied in hospice, oncology, and community health settings.
- She is remembered for her deep empathy, intellectual rigor, and commitment to authentic human connection in nursing.
Major Concepts
Core Philosophical Foundations
- Existentialism: Each person is a unique being with freedom, choice, and responsibility.
- Phenomenology: Focuses on lived experiences and the meaning individuals assign to them.
Concepts
| Concept | Description |
|---|---|
| Person | A unique, dynamic being capable of self-reflection and growth |
| Nursing | A responsible, searching, transactional relationship between nurse and patient |
| Dialogue | The heart of humanistic nursing—an authentic, mutual exchange |
| Presence | Being fully engaged and emotionally available in the moment |
| Responsibility | Nurses must be aware of their own values and choices in each interaction |
Paterson and Zderad viewed nursing as an art and science of human-to-human interaction, where both participants are transformed through the caring process.
Key Concepts
- Human-to-Human Relationship – Nursing is an interactive, interpersonal process.
- Authentic Presence – The nurse must be fully present, genuinely attentive to the patient’s experience.
- Empathic Understanding – Recognizing the patient’s subjective experience without judgment.
- Nurse Growth – The nurse learns and grows from every authentic interaction.
Five phases of the nursing process:
- Preparation of the Nurse Knower for Coming to Know:
In this stage the nurse acts as investigator who willingly takes risks and has an open-mind. The nurse must be a risk-taker and be willing to experience anything. “Accepting the decision to approach the unknown openly”. - Nurse Knowing of the Other Intuitively:
In this stage the nurse tries to understand the other, as in the “I-thou” relationship, where the nurse as the “I” does not superimpose themselves on the “thou” of the patient. - Nurse Knowing the Other Scientifically:
The nurse as the observer must observe and analyze from the outside. At this stage, the nurse goes from intuition to analysis. Analysis is the sorting, comparing, contrasting, relating, interpreting and categorizing. - Nurse Complementarily Synthesizing Known Others:
The ability of the nurse to develop or see themselves as a source of knowledge, to continually develop the nursing community through education, and increased understanding of their owned learned experiences. - Succession Within the Nurse from the Many to the Paradoxical One:
In this stage the nurse takes the information gleaned and applies it in the practical clinical setting. Here the nurse takes brings the dilemma towards resolution.
Application of Paterson & Zderad’s Humanistic Nursing Theory
- Establish Therapeutic Relationships
- Develop trust and rapport by being authentically present and listening attentively.
- Provide Holistic, Human-Centered Care
- Focus not only on the physical illness but also on emotional, spiritual, and psychosocial needs.
- Empathetic Communication
- Use active listening, nonverbal cues, and reflective responses to truly understand patient concerns.
- Mutual Growth and Reflection
- Recognize that nursing care is transformative for both the patient and the nurse.
- Integration with Clinical Interventions
- Combine technical and procedural care with humanistic interactions to promote healing.
Case Scenario 1: Terminally Ill Patient in Hospice Care
Scenario:
Mr. A, 68 years old, with end-stage lung cancer, is in a hospice facility. He expresses fear of dying alone and emotional distress about leaving his family.
Assessment
- Verbalizes fear and sadness
- Withdrawn, tearful, and restless at night
- States: “I don’t want to die alone.”
Nursing Diagnoses
- Anticipatory grieving related to terminal illness.
- Spiritual distress related to fear of death and separation from family.
Nursing Interventions (Humanistic Nursing Approach)
- Be authentically present – Sit quietly with the patient, hold their hand, and allow expression of feelings without interruption.
- Active listening and empathy – Validate patient’s fears and encourage life reflection.
- Facilitate family interaction – Arrange family visits or video calls to reduce emotional isolation.
- Integrate spiritual care – Offer chaplain or spiritual counselor if patient desires.
Expected Outcome:
- Patient verbalizes reduced fear and emotional relief.
- Experiences meaningful family connection and spiritual comfort.
Case Scenario 2: Young Adult with Depression and Social Withdrawal
Scenario:
Ms. B, 24 years old, admitted for major depressive episode. She isolates herself, avoids eye contact, and has feelings of worthlessness.
Assessment
- Minimal verbal communication
- Poor eye contact and flat affect
- States: “No one cares about me anymore.”
Nursing Diagnoses
- Social isolation related to depression and low self-esteem.
- Hopelessness related to altered perception of self-worth.
Nursing Interventions (Humanistic Nursing Approach)
- Establish a trusting relationship – Spend unhurried time, gently initiate conversation.
- Provide empathic support – Validate her emotions without judgment; use reflective listening.
- Encourage self-expression – Through art, journaling, or talking to gradually rebuild connection.
- Facilitate support systems – Encourage group therapy or family involvement to enhance social interaction.
Expected Outcome:
- Patient demonstrates improved willingness to interact with staff and peers.
- Expresses less hopelessness and engages in simple activities.
REFERENCES
- Kleiman, S. (2010). Josephine Paterson and Loretta Zderad’s humanistic nursing theory. In M. E. Parker & M. C. Smith (Eds.), Nursing theories and nursing practice (3rd ed., pp. 337-350). Philadelphia: F. A. Davis.
- Paterson, J. G., & Zderad, L. T. (1976). Humanistic nursing. New York, NY: Wiley.
- Oldnall, A. (1993), Paterson and Zderad: Humanistic Nursing Theory. Journal of Advanced Nursing, 18: 1850-1850. https://doi.org/10.1046/j.1365-2648.1993.181118494.x
- Silva TN. Paterson and Zderad’s humanistic theory: entering the between through being when called upon. Nurs Sci Q. 2013 Apr;26(2):132-5. https://pubmed.ncbi.nlm.nih.gov/23575489/
- Wolf, Z. R., & Bailey, D. N.. (2013). Paterson and Zderad’s humanistic nursing theory: Concepts and applications. International Journal for Human Caring, 17(4), 60–69.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


