


Carotid artery dissection occurs when there is a tear or separation in the layers of the carotid artery in your neck. There are two carotid arteries, one on each side of your neck. Dissection can occur spontaneously or after a neck injury. The condition can heal itself over time but may cause life-threatening complications, such as stroke or bleeding in the brain.
Introduction
Carotid artery dissection (CAD) is a significant vascular condition that affects the carotid arteries, which are critical suppliers of blood to the brain. This disease, though relatively uncommon, is a leading cause of stroke, especially in younger adults and middle-aged individuals. Understanding CAD is essential for medical professionals, as timely diagnosis and appropriate management can be life-saving and prevent long-term neurological deficits. This article provides a comprehensive overview of carotid artery dissection, covering its definition, epidemiology, aetiology, risk factors, pathophysiology, clinical presentation, diagnostic modalities, management strategies, complications, prognosis, and recent advances in the field.
Definition and Epidemiology
Definition
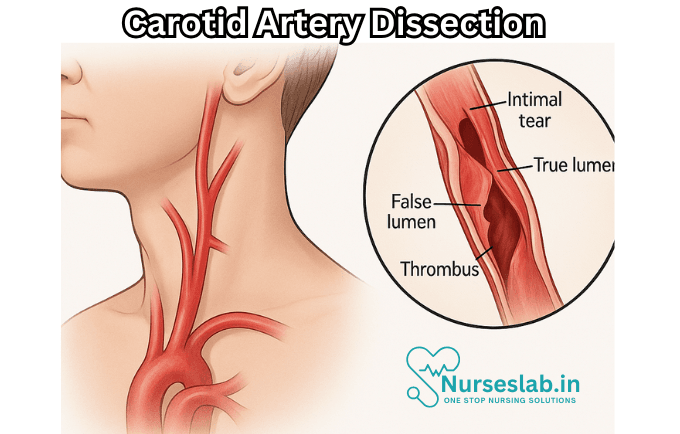
Carotid artery dissection refers to a tear or separation within the layers of the carotid artery wall, most often the internal carotid artery. This process allows blood to enter the arterial wall, creating a false lumen which may lead to stenosis, occlusion, or even aneurysm formation. The dissection can compromise cerebral blood flow and facilitate thromboembolism, resulting in transient ischaemic attacks (TIAs) or ischaemic stroke.
Epidemiology
CAD accounts for approximately 2% of all ischaemic strokes, but it is responsible for up to 20–25% of strokes in individuals under the age of 45. The estimated annual incidence ranges between 2.5 to 3 cases per 100,000 people for spontaneous cervical artery dissections, with a slight male predominance. The mean age of onset is around 45 years, but cases have been reported across a wide age spectrum, including adolescents and the elderly. Both spontaneous and traumatic forms of CAD exist, with spontaneous cases being more common.
Etiology and Risk Factors
Causes
Carotid artery dissection can occur spontaneously or as a consequence of trauma. Traumatic dissections are often associated with blunt or penetrating injuries to the neck, rapid deceleration accidents, or iatrogenic causes such as surgical or interventional procedures. Spontaneous dissections may be precipitated by minor trauma, sudden neck movements, or may occur without any identifiable external cause.
Genetic and Acquired Risk Factors
- Connective Tissue Disorders: Conditions such as Ehlers-Danlos syndrome (particularly type IV), Marfan syndrome, and fibromuscular dysplasia are associated with an increased risk due to inherent vessel wall fragility.
- Genetic Predisposition: Certain polymorphisms, such as those in the COL3A1 gene, may predispose individuals to arterial dissection.
- Hypertension: Chronic high blood pressure can weaken arterial walls.
- Migraine: Some studies suggest a higher prevalence of CAD among migraine sufferers, potentially due to underlying vascular abnormalities.
- Smoking: Tobacco use is a modifiable risk factor that can contribute to vascular injury.
- Infections: Recent respiratory tract infections have been identified as potential triggers, possibly due to inflammatory processes affecting the vessel wall.
- Hyperhomocysteinaemia: Elevated homocysteine levels may be associated with increased susceptibility.
- Hormonal Factors: Use of oral contraceptives and pregnancy have been implicated in some cases.
- Physical Trauma: Even minor trauma such as coughing, sneezing, or chiropractic manipulation can precipitate dissection in susceptible individuals.
Pathophysiology
The fundamental event in carotid artery dissection is a tear in the intimal layer of the artery, allowing blood to enter the subintimal or subadventitial space. This creates a false lumen and can result in the formation of an intramural haematoma. The expanding haematoma may compress the true lumen, leading to arterial stenosis or occlusion. Alternatively, the dissection may extend longitudinally, affecting a longer arterial segment.
The pathophysiological consequences include:
- Arterial Narrowing or Occlusion: Compression of the true lumen reduces cerebral perfusion, increasing the risk of ischaemia.
- Thrombus Formation: Disruption of the endothelial surface promotes local thrombosis, which may embolise distally causing TIAs or stroke.
- Pseudoaneurysm Formation: The weakened arterial wall may bulge outward, forming a pseudoaneurysm with risk of rupture or further embolic events.
- Inflammatory Response: Secondary inflammation may exacerbate vascular injury and contribute to symptoms.
Clinical Presentation
The clinical features of carotid artery dissection are variable and can mimic other neurological or vascular disorders. The classic triad includes unilateral neck pain or headache, partial Horner’s syndrome (ptosis, miosis, anhidrosis), and cerebral or retinal ischaemia. However, all three features are present in only a minority of cases.
Signs and Symptoms
Local Symptoms:
- Unilateral neck pain or facial pain, often sudden in onset and severe.
- Headache, typically in the temporal or periocular region.
- Horner’s syndrome due to disruption of sympathetic fibres.
- Pulsatile tinnitus or bruit over the carotid artery.
- Cranial nerve palsies, especially IX, X, XI, and XII, due to compression or ischaemia.
Cerebral Ischaemia:
- Transient ischaemic attacks (TIAs).
- Ischaemic stroke, manifesting as hemiparesis, aphasia, visual disturbances, or other focal deficits.
- Amaurosis fugax (transient monocular blindness) due to retinal embolism.
Other Features:
- Scalp tenderness.
- Audible bruit in the neck.
- Symptoms may evolve over hours to days.
It is important to note that some patients may present with only mild symptoms or may be asymptomatic, with the dissection discovered incidentally on imaging.
Diagnosis
Prompt and accurate diagnosis of carotid artery dissection is essential to guide management and prevent complications. Diagnosis is primarily based on imaging studies, supported by clinical findings.
Imaging Modalities
Magnetic Resonance Imaging (MRI) and Magnetic Resonance Angiography (MRA):
- MRI is highly sensitive for detecting intramural haematoma and vessel wall changes.
- MRA provides detailed images of the arterial lumen, identifying stenosis, occlusion, or pseudoaneurysm formation.
Computed Tomography Angiography (CTA):
- Rapid, widely available, and excellent for assessing both the vessel lumen and wall.
- Useful in acute settings and in patients unable to undergo MRI.
Duplex Ultrasonography:
- Non-invasive and can detect flow abnormalities, stenosis, or occlusion.
- Limited sensitivity for distal or petrous carotid dissections.
Digital Subtraction Angiography (DSA):
- Gold standard for vascular imaging but invasive and reserved for equivocal cases or when endovascular intervention is considered.
Laboratory Findings
There are no specific laboratory tests for carotid artery dissection. Workup may include basic blood investigations, coagulation profile, markers of inflammation, and screening for underlying connective tissue disorders or hypercoagulable states, especially in young or recurrent cases.
Differential Diagnosis
- Other causes of stroke or TIA (e.g., cardioembolism, atherosclerosis).
- Migraine with aura.
- Cluster headache.
- Giant cell arteritis.
- Cervical radiculopathy.
- Vasculitis.
- Infectious or neoplastic processes affecting the neck.
Management and Treatment
The management of carotid artery dissection aims to prevent stroke, minimise neurological deficits, and promote arterial healing. Treatment strategies are individualised based on the patient’s clinical presentation, severity of dissection, and presence of complications.
General Principles
Early diagnosis and initiation of treatment are crucial. Multidisciplinary management involving neurology, vascular surgery, radiology, and sometimes cardiology is often required.
Medical Management
Antithrombotic Therapy:
- Antiplatelet agents (aspirin, clopidogrel) or anticoagulation (heparin, warfarin) are commonly used to reduce the risk of thromboembolism.
- The choice between antiplatelets and anticoagulants is debated; both are considered effective, and current guidelines recommend either based on individual risk profiles.
- Duration of therapy is typically 3–6 months, followed by reassessment.
Blood Pressure Management:
- Strict control of blood pressure to prevent extension or recurrence of dissection.
Pain Management:
- Analgesics for symptomatic relief of headache and neck pain.
Treatment of Underlying Disorders:
- Addressing connective tissue disorders, hypercoagulable states, or other predisposing conditions.
Endovascular and Surgical Interventions
Endovascular Therapy:
- Indicated for patients with persistent or worsening neurological symptoms despite medical management, or with haemodynamically significant arterial stenosis or pseudoaneurysm.
- Procedures include stenting of the dissected segment or coiling of pseudoaneurysms.
Surgical Intervention:
- Rarely required, reserved for complex cases not amenable to endovascular techniques.
- Options include bypass grafting or surgical repair of the dissected artery.
Rehabilitation
Patients with neurological deficits benefit from early and comprehensive rehabilitation, including physical, occupational, and speech therapy as indicated. Psychological support may be necessary for those with significant morbidity.
Complications
Carotid artery dissection can lead to various complications, both acute and chronic.
- Stroke: The most serious complication, resulting from thromboembolism or haemodynamic compromise.
- Transient Ischaemic Attacks: Temporary neurological deficits due to transient vascular occlusion.
- Pseudoaneurysm Formation: Risk of rupture, further embolic events, or local compression of adjacent structures.
- Recurrent Dissection: Especially in patients with underlying connective tissue disorders.
- Cranial Nerve Palsies: Due to mass effect or ischaemia.
- Chronic Headache or Neck Pain: Persistent symptoms in some patients even after arterial healing.
Prognosis
The prognosis for carotid artery dissection has improved significantly with advances in diagnostic imaging and early intervention. Most patients experience good recovery, especially if treatment is initiated promptly and there are no major ischaemic complications. However, outcomes depend on the severity of initial neurological involvement, extent of arterial injury, and presence of comorbidities.
- Recurrence: Estimated recurrence rates are low (around 1% per year), but higher in those with predisposing connective tissue disorders.
- Long-Term Follow-Up: Regular clinical and imaging follow-up is recommended to monitor for arterial healing, recurrence, or delayed complications such as pseudoaneurysm formation.
- Quality of Life: Most patients return to baseline function, although a minority may have persistent deficits or require long-term rehabilitation.
Nursing Care of Patients with Carotid Artery Dissection
The management of patients with carotid artery dissection requires a multidisciplinary approach, with nurses playing a pivotal role in both acute and long-term care.
Nursing Assessment
Nursing assessment forms the foundation for effective care planning and intervention in patients with carotid artery dissection.
Comprehensive Evaluation
- Obtain a thorough history, focusing on the onset, duration, and characteristics of symptoms.
- Assess for recent trauma, underlying medical conditions, and family history of vascular disorders.
- Perform detailed neurological assessments, including cranial nerve evaluation, motor and sensory testing, and level of consciousness.
- Monitor vital signs with particular attention to blood pressure, as hypertension can exacerbate dissection.
- Observe for signs of stroke or transient ischemic attacks: sudden numbness, weakness, confusion, visual disturbances, or difficulty speaking.
- Evaluate pain levels, location, and response to pain management strategies.
- Monitor for subtle signs of progression, such as new or worsening neurological deficits or changes in mental status.
Diagnostic Procedures
Nurses often assist in preparing patients for diagnostic tests such as:
- Duplex ultrasound of the carotid arteries.
- Magnetic resonance angiography (MRA).
- Computed tomography angiography (CTA).
- Conventional angiography (when indicated).
Nursing Interventions
The primary goals of nursing interventions are to minimize the risk of stroke, manage symptoms, prevent complications, and provide emotional support.
1. Monitoring and Early Detection
- Continuous monitoring of neurological status for early identification of deterioration.
- Frequent assessments of vital signs, especially blood pressure and heart rate.
- Observation for complications such as hematoma, airway compromise, or extension of the dissection.
- Prompt reporting of any changes in neurological or cardiovascular status to the medical team.
2. Blood Pressure Management
- Maintain blood pressure within the target range as prescribed to reduce further arterial wall damage.
- Administer antihypertensive medications as ordered and monitor for effectiveness and adverse effects.
- Educate the patient and family on the importance of blood pressure control and adherence to medication regimens.
3. Pain Management
- Administer analgesics as prescribed to relieve neck pain or headache.
- Use non-pharmacologic interventions, such as ice packs, relaxation techniques, or gentle positioning, to reduce discomfort.
- Regularly assess pain levels and adjust interventions as needed.
4. Antithrombotic Therapy Support
- Administer anticoagulants or antiplatelet agents as prescribed to prevent thromboembolic complications.
- Monitor for signs of bleeding, bruising, or changes in hemoglobin/hematocrit.
- Educate the patient about potential side effects and signs that require immediate attention (e.g., unexplained bruising, hematuria, or gastrointestinal bleeding).
5. Neurological Protection and Stroke Prevention
- Promote a calm, quiet environment to reduce stress and sympathetic stimulation, minimizing the risk of further arterial injury.
- Assist with early mobilization as tolerated, following neurological stabilization and in accordance with physician orders.
- Prevent complications of immobility, such as deep vein thrombosis, pressure ulcers, and pneumonia, by encouraging movement and frequent repositioning.
6. Airway and Respiratory Care
- Monitor for signs of airway compromise due to expanding hematoma or extension of the dissection.
- Be prepared for emergency interventions if respiratory distress develops.
- Encourage deep breathing exercises and coughing to prevent respiratory complications in non-acute cases.
7. Patient and Family Education
Effective communication and education empower patients and families to participate actively in recovery and secondary prevention.
- Explain the nature of carotid artery dissection and the rationale for various treatments and interventions.
- Educate on the importance of medication adherence, follow-up imaging, and lifestyle modifications (e.g., smoking cessation, healthy diet, and exercise).
- Teach recognition of stroke warning signs and when to seek immediate medical help.
- Address emotional needs, concerns, and anxieties related to diagnosis and prognosis.
8. Discharge Planning and Long-Term Management
- Coordinate multidisciplinary team involvement for rehabilitation, physical therapy, occupational therapy, and speech therapy as needed.
- Arrange follow-up appointments for imaging studies and specialist reviews.
- Provide written instructions and resources for ongoing self-care and monitoring at home.
- Support reintegration into work, social, and family life, addressing any limitations or accommodations required.
Special Considerations
Pediatric Patients
Carotid artery dissection, though rare in children, requires tailored nursing approaches, including age-appropriate communication, specific assessment tools, and family-centered care.
Pregnant or Postpartum Individuals
CAD during or after pregnancy presents unique risks; nurses must closely monitor for symptoms and collaborate with obstetric teams for optimal maternal and fetal outcomes.
Patients with Underlying Connective Tissue Disorders
These individuals may require close monitoring for recurrent dissections or additional vascular complications.
Psychosocial Support
Nurses should assess and address the emotional and psychological impact of a sudden neurological event. Counseling services, peer support groups, and involvement of clinical psychologists can be beneficial in managing anxiety, depression, or adjustment difficulties.
Collaboration and Communication
Effective care for patients with CAD relies on seamless communication between nurses, physicians, radiologists, pharmacists, therapists, and social workers. Regular multidisciplinary rounds ensure coordinated care plans and optimal outcomes.
Ethical and Legal Aspects
Nurses must maintain patient confidentiality, obtain informed consent for procedures, and advocate for patient rights. Shared decision-making and respect for patient autonomy are essential in complex cases where treatment options may carry significant risks.
REFERENCES
- Blum CA, Yaghi S. Cervical Artery Dissection: A Review of the Epidemiology, Pathophysiology, Treatment, and Outcome. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4604565/. Arch Neurosci. 2015;2(4):e26670.
- Goodfriend SD, Tadi P, Koury R. Carotid Artery Dissection. https://www.ncbi.nlm.nih.gov/books/NBK430835/. [Updated 24 Dec 2021]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
- Radiopaedia. Internal carotid artery dissection. https://radiopaedia.org/articles/internal-carotid-artery-dissection-1?lang=us.
- Goodfriend SD, Tadi P, Koury R. Carotid Artery Dissection. [Updated 2022 Dec 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430835/
- Wood EC, Marcet PA, Fargen KM, Velazquez-Ramirez G. Contemporary Management and Outcomes of Carotid Artery Dissection. Ann Vasc Surg. 2025 Apr;113:406-414. doi: 10.1016/j.avsg.2024.06.047. Epub 2024 Sep 27. PMID: 39343363.
- Li T, Lan W, Zhang X, et al. Carotid artery dissection recanalization: imaging modalities, influencing factors, and therapeutic perspectives. Front Neurol. 2025. 16:1624698.
- Ohshima T, Miyachi S, Isaji T, Matsuo N, Kawaguchi R, Takayasu M. Bilateral vertebral artery dissection and unilateral carotid artery dissection in case of Ehlers-Danlos syndrome type IV. World Neurosurg. 2019 Jan. 121:83-7.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


