


Last Updated on January 21, 2026 by Nurseslab.in Editorial Team
Introduction
Chronic Venous Insufficiency (CVI) is a widespread vascular condition that affects millions worldwide, yet its impact is often underestimated in both clinical practice and general awareness. At its core, CVI represents the failure of venous valves and vessels to efficiently return blood from the lower extremities to the heart, leading to pooling, increased venous pressure, and a cascade of symptoms and complications.
Pathophysiology of CVI
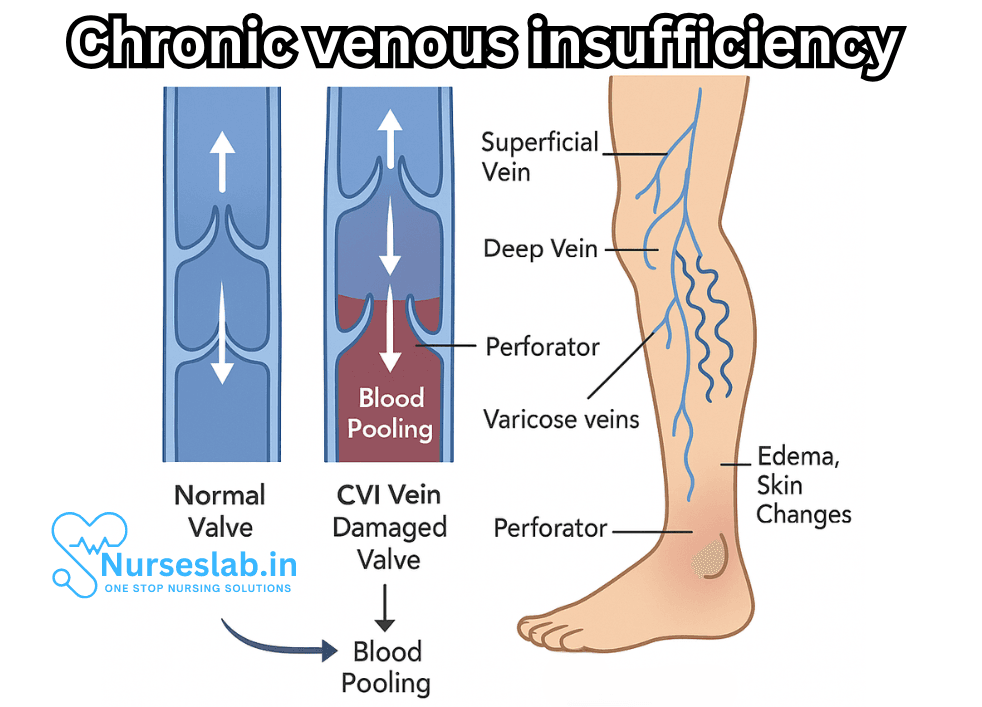
Venous circulation is designed to combat gravity, propelling blood upwards through a network aided by muscular contractions and competent one-way valves. In CVI, these valves become faulty or incompetent, allowing blood to flow backwards (reflux), accumulate, and exert pressure on venous walls. Over time, this increased hydrostatic pressure leads to venous distention, leakage of fluid into surrounding tissues, and chronic inflammation.
Several factors contribute to the development of CVI:
- Valve Dysfunction: The most direct cause, often resulting from genetic predisposition, previous venous thrombosis (such as deep vein thrombosis), or trauma.
- Venous Obstruction: Blockage of veins due to thrombosis, external compression, or intrinsic abnormalities.
- Muscle Pump Failure: Reduced mobility, muscle weakness, or neurological impairment can hinder the calf muscle pump, crucial for venous return.
- Venous Wall Damage: Chronic inflammation or exposure to toxins can degrade the structural integrity of veins, exacerbating valve incompetence.
Risk Factors
CVI arises from an interplay of genetic, lifestyle, and environmental factors. Recognizing these risk factors is essential for early identification and preventive care.
- Age: Incidence increases with age due to cumulative vein damage and reduced tissue resilience.
- Gender: Women are more likely to develop CVI, partly due to hormonal influences and pregnancy-related changes.
- Family History: Genetics play a substantial role, with a positive family history raising predisposition.
- Obesity: Excess weight increases pressure on venous structures and impairs circulation.
- Prolonged Standing or Sitting: Occupations requiring extended periods of immobility increase venous pressure and risk.
- Pregnancy: Hormonal shifts and increased blood volume during pregnancy can contribute to CVI, especially with multiple pregnancies.
- History of Deep Vein Thrombosis (DVT): Previous clot formation can permanently damage valves and veins, precipitating CVI.
Clinical Presentation and Symptoms
CVI typically develops insidiously, with symptoms intensifying as the condition progresses. Common clinical features include:
- Leg Swelling (Edema): Usually worse by day’s end and improves with elevation.
- Heaviness and Fatigue: Patients often report a sensation of heaviness, aching, or tiredness in the legs.
- Pain and Cramps: Aching pain, cramping, or throbbing, especially after prolonged standing.
- Varicose Veins: Enlarged, twisted superficial veins visible under the skin.
- Skin Changes: Hyperpigmentation, eczema, and lipodermatosclerosis (hardening of the skin and subcutaneous tissue).
- Itching and Irritation: Chronic venous stasis can cause pruritus and local discomfort.
- Venous Ulcers: In advanced cases, poorly healing ulcers develop near the ankles, particularly on the medial malleolus.
Stages of CVI
To better guide treatment and prognosis, CVI is classified into stages:
- Stage I: Mild symptoms, including cosmetic changes like spider veins and mild swelling.
- Stage II: Moderate symptoms, such as varicose veins, more pronounced edema, and skin discoloration.
- Stage III: Advanced disease, characterized by chronic pain, significant swelling, skin thickening, and venous ulcers.
Diagnosis
A thorough clinical evaluation, supported by diagnostic testing, is essential for confirming CVI and guiding management.
- Physical Examination: Assessment of leg swelling, skin changes, and varicose veins. The patient is often examined standing to accentuate findings.
- Duplex Ultrasonography: The gold standard non-invasive test for assessing venous reflux, obstruction, and valve competence.
- Venography: Contrast imaging used in select cases for detailed vein mapping.
- Photoplethysmography: Assesses venous function and refill rates.
- Other Tests: Blood tests to rule out clotting disorders, and skin biopsy for unusual or non-healing ulcers.
Management Strategies
Treatment focuses on alleviating symptoms, slowing progression, preventing complications, and improving quality of life. A multidisciplinary approach involving lifestyle modification, medical therapy, and procedural interventions is often necessary.
Lifestyle and Conservative Measures
- Leg Elevation: Encouraging patients to elevate legs above heart level several times daily reduces edema and discomfort.
- Compression Therapy: Graduated compression stockings are foundational, improving venous return and reducing swelling.
- Exercise: Regular walking, cycling, or swimming activates the calf muscle pump and enhances circulation.
- Weight Management: Reducing excess body weight lessens vein pressure.
- Skin Care: Gentle cleansing and moisturizing prevent eczema and ulceration.
Medical Management
- Pharmacological Agents: Venoactive medications (such as flavonoids) may reduce symptoms. Pain, itching, and infection are managed with appropriate analgesics, antihistamines, and antibiotics.
- Treatment of Ulcers: Dressings, topical treatments, and wound care specialists are integral for healing venous ulcers.
Procedural and Surgical Interventions
For those with persistent symptoms or severe disease, interventional therapies may be warranted:
- Endovenous Ablation: Minimally invasive procedures (laser or radiofrequency) to close malfunctioning veins.
- Sclerotherapy: Injection of sclerosing agents to obliterate varicose veins.
- Vein Stripping and Ligation: Surgical removal or tying off affected veins, reserved for severe cases.
- Microphlebectomy: Removal of superficial veins via small incisions.
Complications
If unmanaged, CVI can precipitate significant complications:
- Venous Ulcers: Chronic, painful, and slow-healing wounds prone to infection.
- Cellulitis: Skin and subcutaneous infection, often requiring antibiotics.
- Deep Vein Thrombosis: Formation of blood clots that can migrate and cause pulmonary embolism.
- Chronic Pain and Disability: Reduced mobility and quality of life.
Prevention
Prevention is grounded in risk factor modification and early intervention:
- Regular Physical Activity: Maintains muscle tone and venous circulation.
- Avoid Prolonged Standing or Sitting: Take frequent movement breaks.
- Use Compression Stockings: Especially for those at high risk (pregnant individuals, those with family history, or previous DVT).
- Maintain Healthy Body Weight: Reduces venous pressure.
- Prompt Attention to Leg Injuries: Prevents complications that may worsen CVI.
Living with CVI
CVI is a lifelong condition. With proper management, most individuals can minimize symptoms and maintain an active lifestyle. Education, self-care, and medical follow-up form the cornerstone of long-term success. Support groups, professional counseling, and rehabilitation can further enhance well-being.
Nursing Care of Patients with Chronic Venous Insufficiency (CVI)
Effective nursing care is essential to manage this debilitating condition, promote healing, prevent complications, and improve the quality of life of affected individuals.
Assessment and Diagnosis
Comprehensive Patient Assessment:
Nurses play a pivotal role in the early identification and ongoing assessment of CVI. A thorough patient assessment should include:
- Detailed health history (previous thrombosis, varicose veins, family history, risk factors)
- Physical examination of the lower extremities for swelling, discoloration, varicosities, skin texture (lipodermatosclerosis), and presence of ulcers
- Assessment for pain, heaviness, itching, and cramping in the legs
- Evaluation of mobility and activities of daily living
- Discussion of occupational and lifestyle factors affecting venous return
- Psychosocial assessment, including impact on self-image and mental well-being
Diagnostic Procedures:
Nurses should be familiar with diagnostic tests used to confirm CVI and its severity:
- Doppler ultrasound: to assess venous flow and valve function
- Venography: to visualize veins and identify obstructions or valve incompetence
- Photoplethysmography: to measure venous refill time
Key Nursing Interventions
1. Promoting Venous Return and Reducing Edema
- Leg Elevation: Encourage patients to elevate their legs above heart level several times a day for 15–30 minutes to facilitate venous return and reduce swelling.
- Compression Therapy: Instruct patients on the proper use of graduated compression stockings, which help reduce venous pressure, prevent edema, and promote healing of ulcers. Assess skin integrity regularly to avoid pressure injuries.
- Exercise and Mobility: Advise patients to engage in regular physical activities such as walking, which activates the calf muscle pump and improves circulation. In cases of limited mobility, passive range-of-motion exercises may be beneficial.
- Weight Management: Support patients in maintaining a healthy weight through balanced nutrition and physical activity, as obesity exacerbates CVI symptoms.
2. Skin Care and Ulcer Prevention
- Daily Skin Inspection: Teach patients to inspect their legs and feet daily for signs of injury, infection, or ulceration. Early detection allows for timely intervention.
- Moisturization: Recommend regular application of moisturizers to prevent skin dryness and cracking, which can lead to ulcer formation. Avoid irritants and perfumed lotions.
- Wound Care: For patients with venous ulcers, provide or coordinate evidence-based wound care including gentle cleansing, appropriate dressings, and infection control. Collaborate with wound care specialists when necessary.
- Protection from Trauma: Advise patients to wear protective footwear and avoid activities that could cause leg injuries.
3. Infection Prevention
- Monitoring for Infection: Assess for signs of cellulitis or wound infection (redness, warmth, increased pain, discharge). Early recognition is critical.
- Hygiene Education: Teach patients proper hygiene practices, including gentle washing and thorough drying of lower extremities.
- Prompt Treatment: Ensure timely administration of prescribed antibiotics if infection is suspected.
4. Pain Management
- Pharmacological Measures: Administer analgesics as prescribed, and monitor for effectiveness and side effects.
- Non-Pharmacological Techniques: Teach relaxation methods, elevation, and use of cold packs (if not contraindicated) to relieve discomfort.
5. Patient Education and Self-Management
- Understanding CVI: Provide clear information about the disease process, risk factors, and prognosis to empower patients in self-care.
- Lifestyle Modifications: Advise on dietary changes (low sodium to manage fluid retention), smoking cessation (improves vascular health), and avoiding prolonged standing or sitting.
- Proper Use of Compression Devices: Educate patients on correct application, care, and duration of compression stockings.
- When to Seek Help: Encourage patients to report worsening symptoms, new ulcers, or signs of infection promptly.
Psychosocial Support
CVI can significantly affect mobility, appearance, and self-esteem. Nurses should:
- Provide emotional support and counseling as needed
- Connect patients with support groups and community resources
- Address concerns related to body image and social participation
- Encourage open communication about fears and limitations
Multidisciplinary Collaboration
Optimal CVI management requires a team approach. Nurses coordinate care among:
- Physicians (for medical management and surgical evaluation)
- Physical therapists (for exercise regimens)
- Dietitians (for weight and nutritional guidance)
- Wound care specialists (for complex ulcers)
- Social workers (for psychosocial support and resources)
Preventing Complications
Patients with CVI are at risk for complications such as venous ulcers, skin infections, deep vein thrombosis, and chronic pain. Preventive strategies include:
- Consistent use of compression therapy
- Meticulous skin and wound care
- Regular assessment for changes in the condition
- Patient education for early recognition of complications
Case Management and Follow-up
Long-term management is essential for preventing recurrence and deterioration:
- Regular follow-ups to assess progress and modify care as needed
- Documentation of wound healing, symptom changes, and interventions
- Reinforcement of education and motivation for self-care adherence
- Periodic evaluation for the need of surgical interventions (e.g., vein ablation, sclerotherapy)
REFERENCES
- Chopra A, Liem TK, Moneta GL. Venous and Lymphatic Disease. In: Brunicardi F, Andersen DK, Billiar TR, Dunn DL, Kao LS, Hunter JG, Matthews JB, Pollock RE, eds. Schwartz’s Principles of Surgery. 11th ed. McGraw-Hill; 2019.
- Ghaniwala S, Carman TL. Chronic Venous Insufficiency. In: Walter LC, Chang A, Chen P, Harper G, Rivera J, Conant R, Lo D, Yukawa M, eds. Current Diagnosis & Treatment Geriatrics. 3rd ed. McGraw-Hill; 2021.
- Patel SK, Surowiec SM. Venous Insufficiency. [Updated 2024 Feb 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430975/
- Jayaraj A, Gloviczki P. Chronic Venous Insufficiency. In: Creager MA, Beckman JA, Loscalzo J, eds. Vascular Medicine: A Companion to Braunwald’s Heart Disease. 3rd ed. Elsevier; 2020.
- Merck Manual. Chronic Venous Insufficiency and Postphlebitic Syndrome. https://www.merckmanuals.com/home/heart-and-blood-vessel-disorders/venous-disorders/chronic-venous-insufficiency-and-postphlebitic-syndrome.
- Orhurhu V, Chu R, Xie K, et al. Management of lower extremity pain from chronic venous insufficiency: A comprehensive review. https://pubmed.ncbi.nlm.nih.gov/33704678/. Cardiol Ther. 2021 Jun;10(1):111-140.
- U.S. National Institutes of Health, National Library of Medicine. CEAP Classification of Venous Disorders. https://www.ncbi.nlm.nih.gov/books/NBK557410/.
- Spiridon M, Corduneanu D. Chronic Venous Insufficiency: a Frequently Underdiagnosed and Undertreated Pathology. Maedica (Bucur). 2017 Jan;12(1):59-61. PMID: 28878840; PMCID: PMC5574075.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


