


Last Updated on January 8, 2026 by Nurseslab.in Editorial Team
Cirrhosis of the liver is permanent scarring that damages your liver and interferes with its functioning. It can lead to liver failure. Cirrhosis is the result of persistent liver damage over many years. Alcohol and drugs, viruses and metabolic factors are the most common causes.
Introduction
Cirrhosis of the liver is a chronic, progressive condition characterised by irreversible scarring of the liver tissue, leading to impaired liver function. It represents the final common pathway of multiple liver diseases and is a significant cause of morbidity and mortality worldwide. The liver, a vital organ responsible for metabolism, detoxification, and synthesis of essential proteins, becomes structurally and functionally compromised in cirrhosis. The condition develops gradually, often over years, and may remain asymptomatic until advanced stages.
Causes and Risk Factors
Alcohol Consumption
Excessive and prolonged consumption of alcohol is one of the leading causes of cirrhosis worldwide. Alcohol is metabolised in the liver, and chronic exposure leads to inflammation, fatty changes (steatosis), and eventually fibrosis and cirrhosis. People who consume large quantities of alcohol over several years are at a particularly high risk. The threshold for liver damage varies among individuals, but drinking more than 40-60 grams of alcohol per day is considered especially hazardous.
Chronic Viral Hepatitis
Hepatitis B and hepatitis C viruses are significant contributors to the development of cirrhosis. These viruses cause chronic inflammation and injury to the liver cells. Over time, repeated cycles of cell death and regeneration lead to scarring and loss of normal liver architecture. Hepatitis C is especially notorious for its silent progression, often leading to cirrhosis decades after the initial infection.
Metabolic Diseases
Certain metabolic conditions, such as non-alcoholic fatty liver disease (NAFLD) and its more severe form, non-alcoholic steatohepatitis (NASH), are increasingly recognised as causes of cirrhosis. These conditions are strongly associated with obesity, diabetes mellitus, dyslipidaemia, and insulin resistance. Genetic disorders like haemochromatosis (iron overload) and Wilson’s disease (copper accumulation) also predispose individuals to cirrhosis.
Autoimmune and Other Causes
Autoimmune hepatitis, in which the body’s immune system attacks liver cells, can lead to cirrhosis if not adequately controlled. Primary biliary cholangitis and primary sclerosing cholangitis are other autoimmune disorders affecting the bile ducts, eventually resulting in cirrhosis. Long-term exposure to certain drugs, toxins, and infections such as schistosomiasis may also contribute to the development of hepatic cirrhosis.
Risk Factors
- Chronic alcohol abuse
- History of viral hepatitis infection (especially B and C)
- Obesity and metabolic syndrome
- Family history of liver diseases
- Exposure to hepatotoxic drugs and chemicals
- Autoimmune disorders
Pathophysiology
Cirrhosis results from sustained injury to the liver, triggering inflammatory and fibrotic responses. The normal liver structure comprises lobules made up of hepatocytes, sinusoids, and portal tracts. Persistent injury, whether due to alcohol, viruses, or other causes, leads to the activation of hepatic stellate cells, which transform into fibrous tissue-producing myofibroblasts. This process replaces healthy liver cells with scar tissue, distorting the organ’s architecture and forming regenerative nodules. Blood flow through the liver is subsequently impeded, causing increased pressure in the portal vein (portal hypertension) and impairing critical liver functions such as protein synthesis, detoxification, and metabolism.
Symptoms and Stages
Early Symptoms
In its early stages, cirrhosis may be asymptomatic or present with subtle, non-specific symptoms. These include:
- Fatigue
- Loss of appetite
- Nausea
- Unintentional weight loss
- Mild abdominal discomfort
Advanced Symptoms
As cirrhosis progresses, symptoms become more pronounced and reflect declining liver function. Common features include:
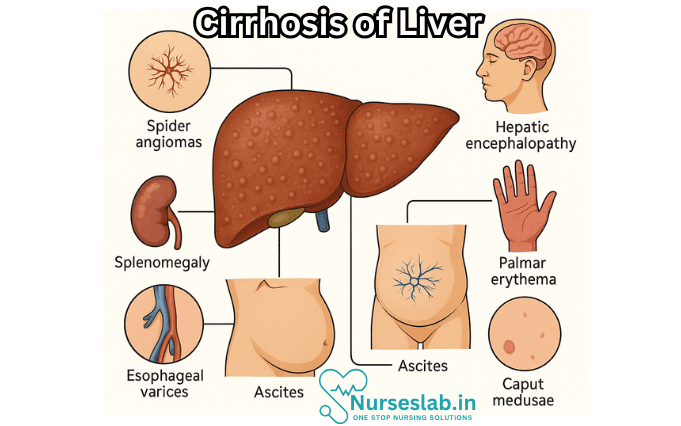
- Jaundice (yellowing of the skin and eyes)
- Swelling of the legs (oedema) and abdomen (ascites)
- Easy bruising and bleeding
- Itchy skin (pruritus)
- Spider angiomas (small, spider-like blood vessels on the skin)
- Muscle wasting
- Confusion or altered mental status (hepatic encephalopathy)
Staging Systems
Cirrhosis is staged based on the severity of liver dysfunction and the presence of complications. The Child-Pugh score and Model for End-Stage Liver Disease (MELD) score are commonly used. The Child-Pugh score evaluates parameters such as bilirubin, albumin, prothrombin time, ascites, and encephalopathy, classifying patients into Class A (least severe), B, or C (most severe). The MELD score uses laboratory values to predict mortality risk and prioritise patients for liver transplantation.
Diagnosis
Clinical Evaluation
Diagnosis begins with a thorough history and physical examination. Physicians look for risk factors, symptoms, and signs suggestive of chronic liver disease, such as jaundice, ascites, spider angiomas, and hepatomegaly (enlarged liver).
Laboratory Tests
- Liver Function Tests: Assess levels of enzymes (ALT, AST), bilirubin, albumin, and clotting factors.
- Complete Blood Count (CBC): May reveal anaemia, low platelet count, and other abnormalities.
- Viral Serology: Tests for hepatitis B and C.
- Autoimmune Markers: Useful if autoimmune hepatitis is suspected.
- Metabolic Panels: To identify metabolic causes like iron or copper overload.
Imaging
Ultrasound is a first-line imaging modality for assessing liver size, texture, and the presence of nodules, ascites, or portal hypertension. More advanced techniques include CT scans and MRI, which provide detailed views of liver anatomy and help detect complications such as hepatocellular carcinoma (liver cancer).
Liver Biopsy
A liver biopsy, though invasive, remains the gold standard for confirming cirrhosis and determining its cause. The procedure involves obtaining a small sample of liver tissue for microscopic examination, allowing assessment of the degree of fibrosis and architectural distortion.
Treatment Options
Medical Management
The primary goal of treatment is to halt or slow disease progression, manage symptoms, and prevent complications. There is no cure for established cirrhosis except for liver transplantation; however, medical management can significantly improve quality of life and survival.
- Managing Underlying Cause: Abstinence from alcohol, antiviral therapy for hepatitis, or treatment of metabolic disorders.
- Symptomatic Management: Diuretics for oedema and ascites; lactulose for hepatic encephalopathy; vitamin supplementation.
- Prevention of Complications: Regular screening for varices and hepatocellular carcinoma; antibiotics for infections; vaccines to prevent hepatitis A and B.
Lifestyle Changes
Patients are advised to adopt healthy lifestyle modifications, including:
- Complete abstinence from alcohol
- Balanced, nutritious diet with adequate protein
- Weight management and regular physical activity
- Avoidance of hepatotoxic medications and substances
Surgical Interventions and Liver Transplantation
In cases of advanced cirrhosis with life-threatening complications, surgical procedures such as transjugular intrahepatic portosystemic shunt (TIPS) may be performed to reduce portal hypertension. Liver transplantation is the definitive treatment for end-stage disease. Selection for transplantation is based on severity scores, overall health, and absence of contraindications. Post-transplant survival rates are generally favourable, although lifelong immunosuppression is required.
Complications
Portal Hypertension
Scarring of liver tissue increases resistance to blood flow, resulting in elevated pressure in the portal vein. This can lead to the formation of varices (dilated veins) in the oesophagus and stomach, which are prone to life-threatening bleeding.
Ascites
Accumulation of fluid in the abdomen due to increased pressure and reduced protein synthesis is a hallmark of decompensated cirrhosis. Ascites increases the risk of infection (spontaneous bacterial peritonitis) and can cause discomfort and respiratory issues.
Hepatic Encephalopathy
Impaired liver function leads to accumulation of toxins, especially ammonia, in the bloodstream. This affects brain function, causing confusion, personality changes, and in severe cases, coma.
Varices and Bleeding
Oesophageal and gastric varices may rupture, resulting in severe gastrointestinal bleeding. This is a medical emergency requiring prompt intervention.
Increased Cancer Risk
Patients with cirrhosis are at significantly increased risk of developing hepatocellular carcinoma. Regular surveillance with imaging and tumour markers is essential for early detection.
Prevention Strategies
Preventing cirrhosis involves addressing modifiable risk factors and promoting liver health. Key strategies include:
- Limiting or abstaining from alcohol consumption
- Vaccination against hepatitis B
- Safe practices to avoid hepatitis transmission (e.g., safe injection, screening of blood products)
- Maintaining a healthy weight and managing diabetes
- Regular medical check-ups for those at risk
- Avoidance of unnecessary use of hepatotoxic drugs
- Early intervention for treatable liver diseases
Prognosis and Quality of Life
The outlook for individuals with cirrhosis depends on the stage at diagnosis, underlying cause, and effectiveness of management. Early-stage cirrhosis can be stabilised with appropriate interventions, whereas advanced disease is associated with a poorer prognosis. Survival rates are often estimated using the Child-Pugh and MELD scores. With optimal medical care, some patients may live for many years, while others progress rapidly to liver failure.
Quality of life can be significantly affected due to physical symptoms, psychological distress, and social limitations. Support from healthcare professionals, family, and patient support groups plays a crucial role. Long-term management focuses on symptom control, complication prevention, regular monitoring, and, when appropriate, preparation for transplantation.
Nursing Care of Patients with Cirrhosis of the Liver
Nursing care for patients with cirrhosis is multifaceted, focusing on symptom management, complication prevention, patient education, and psychosocial support.
1. Assessment and Monitoring
Nurses play a crucial role in the ongoing assessment of patients with cirrhosis to detect changes in condition and prevent complications.
- Vital Signs: Monitor for signs of infection (fever, tachycardia), hypotension (which can indicate bleeding or shock), and tachypnea (possibly related to hepatic encephalopathy or ascites).
- Physical Examination: Assess for jaundice, ascites, peripheral edema, spider angiomata, palmar erythema, and muscle wasting. Note any bruising or bleeding tendencies.
- Neurological Status: Observe for changes in mental status, confusion, irritability, or asterixis, which can signal hepatic encephalopathy.
- Abdominal Assessment: Monitor for increasing abdominal girth (ascites), tenderness, or signs of infection such as spontaneous bacterial peritonitis (rebound tenderness, fever).
- Laboratory Values: Monitor liver function tests (ALT, AST, ALP, bilirubin), coagulation profiles (INR, PT, aPTT), serum albumin, renal function (BUN, creatinine), and electrolytes.
2. Management of Fluid Volume and Ascites
Ascites, or accumulation of fluid in the peritoneal cavity, is a hallmark complication of cirrhosis.
- Daily Weights and Abdominal Girth Measurements: Track changes to monitor fluid retention or loss.
- Fluid and Sodium Restriction: Collaborate with dietary services to restrict sodium (typically to <2g/day) and fluids as ordered.
- Diuretic Therapy: Administer diuretics (spironolactone, furosemide) as prescribed and monitor for electrolyte imbalances (hypokalemia, hyponatremia).
- Skin Integrity: Ascites and edema can increase risk for skin breakdown. Reposition frequently, use pressure-relieving devices, and keep skin clean and dry.
- Paracentesis: Prepare for and assist with abdominal paracentesis when indicated. Monitor for hypotension and infection post-procedure.
3. Prevention and Management of Hepatic Encephalopathy
Hepatic encephalopathy (HE) is a neuropsychiatric disorder resulting from the accumulation of toxins (primarily ammonia) due to impaired hepatic function.
- Neurological Assessment: Monitor for subtle changes in cognitive function or personality, progressing to drowsiness, stupor, or coma if untreated.
- Lactulose Administration: Administer lactulose as prescribed to reduce blood ammonia levels, titrating dose to achieve 2-3 soft stools per day.
- Avoid Constipation: Encourage adequate fiber intake if not contraindicated, and monitor bowel patterns closely.
- Medication Review: Avoid sedatives, opioids, or other CNS depressants unless absolutely necessary and prescribed.
- Dietary Protein: Collaborate with dietitians for optimal protein intake, as restriction is now limited and must be individualized.
- Patient Safety: Institute fall precautions due to confusion or weakness, and orient patient to environment regularly.
4. Bleeding Precautions
Cirrhosis impairs the synthesis of clotting factors, increasing the risk of bleeding and bruising.
- Monitor for Bleeding: Assess for signs of GI bleeding (hematemesis, melena), bleeding gums, epistaxis, and easy bruising.
- Minimize Trauma: Use soft toothbrushes and electric razors, avoid intramuscular injections when possible, apply gentle pressure to venipuncture sites.
- Monitor Laboratory Values: Pay close attention to platelet count and coagulation profile for early detection of coagulopathy.
- Prepare for Blood Transfusion: Be prepared to administer blood products as ordered if significant bleeding occurs.
5. Nutritional Support
Proper nutrition is vital in managing cirrhosis, as malnutrition is common and worsens prognosis.
- Caloric and Protein Intake: Provide high-calorie, high-protein diet unless protein restriction is indicated due to hepatic encephalopathy.
- Small, Frequent Meals: Encourage small, frequent meals and snacks to reduce fatigue and encourage intake.
- Vitamin and Mineral Supplementation: Administer vitamin supplements, particularly vitamins A, D, E, K, and B complex, as prescribed.
- Monitor for Anorexia and Nausea: Offer appealing food options; manage nausea and vomiting as appropriate.
6. Infection Prevention
Patients with cirrhosis are immunocompromised and at increased risk for infections, especially spontaneous bacterial peritonitis and respiratory infections.
- Hand Hygiene and Aseptic Techniques: Practice strict hand hygiene and aseptic technique for all procedures.
- Monitor for Infection: Assess for fever, leukocytosis, changes in mental status, or new-onset abdominal pain.
- Vaccination: Encourage influenza and pneumococcal vaccinations; hepatitis A and B vaccination if not already immune.
- Patient Education: Teach about signs of infection and when to seek medical attention promptly.
7. Skin Care and Comfort Measures
Cirrhosis and its complications (jaundice, edema, pruritus) can severely affect skin integrity and patient comfort.
- Pruritus Management: Provide antihistamines or topical agents for itching; maintain cool, moist environment.
- Skin Protection: Avoid adhesive tapes when possible, keep fingernails trimmed, and encourage loose-fitting clothing.
- Pressure Ulcer Prevention: Reposition bedridden patients every 2 hours and use pressure-relieving surfaces.
8. Education and Psychosocial Support
Chronic illness significantly impacts the psychological well-being of patients and families.
- Disease Process Education: Provide clear explanations about cirrhosis, its progression, and management options.
- Medication Adherence: Teach importance of taking medications as prescribed and reporting side effects.
- Lifestyle Modifications: Counsel on the need for alcohol cessation, smoking cessation, and adherence to dietary restrictions.
- Support Groups and Counseling: Refer to support groups, social workers, or counseling services as needed for coping and adjustment.
- Advance Care Planning: Discuss prognosis, palliative care options, and facilitate advance directives when appropriate.
9. Collaboration and Interdisciplinary Care
Care for patients with cirrhosis is best provided through interdisciplinary collaboration:
- Work closely with physicians, dietitians, pharmacists, physical therapists, and social workers.
- Coordinate discharge planning and community support services.
10. Prevention of Acute Complications
Vigilance for acute complications is essential:
- Variceal Bleeding: Monitor for signs of upper GI bleeding, and administer vasoactive drugs or prepare for endoscopic interventions as ordered.
- Hepatorenal Syndrome: Assess renal function and urine output; notify provider of sudden changes.
- Spontaneous Bacterial Peritonitis: Promptly recognize abdominal pain, tenderness, or fever, and facilitate diagnostic paracentesis where indicated.
REFERENCES
- American Liver Foundation. Cirrhosis of the Liver ., https://liverfoundation.org/liver-diseases/complications-of-liver-disease/cirrhosis/. Updated 6/12/2025.
- Feldman M, et al., eds. Overview of cirrhosis. In: Sleisenger and Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology, Diagnosis, Management. 11th ed. Elsevier; 2021. https://www.clinicalkey.com.
- National Institute of Diabetes and Digestive and Kidney Diseases (U.S.). Cirrhosis ., https://www.niddk.nih.gov/health-information/liver-disease/cirrhosis. Updated 6/2023.
- Sharma B, John S. Hepatic Cirrhosis ., https://www.ncbi.nlm.nih.gov/books/NBK482419/. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan. Updated 2022 Oct 31.
- Tonon M, et al. Acute on chronic liver failure in cirrhosis. Clinical and Molecular Hepatology. 2022; doi:10.3350/cmh.2022.0036.
- Jophlin LL, et al. ACG clinical guideline: Alcohol-associated liver disease. The American Journal of Gastroenterology. 2024; doi:10.14309/ajg.0000000000002572.
- Simon TG, Kim MN, Luo X, et al. Physical activity compared to adiposity and risk of liver-related mortality: results from two prospective, nationwide cohorts. J Hepatol. 2020;72(6):1062-1069. doi:10.1016/j.jhep.2019.12.022
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


