


Last Updated on January 12, 2026 by Nurseslab.in Editorial Team
Introduction
Laminectomy is a surgical procedure primarily aimed at relieving pressure on the spinal cord or nerves caused by stenosis, herniated discs, bone spurs, or tumors. As one of the most common forms of spinal decompression surgery, it plays a crucial role in the management of chronic back pain and neurological deficits that fail to respond to conservative treatment.
Anatomy of the Spine
The spine is composed of a series of vertebrae stacked one on top of another, separated by intervertebral discs. Each vertebra consists of several parts, including the vertebral body, pedicles, laminae, spinous process, and articular processes. The laminae are flat, thin sections of bone that form the roof of the vertebral arch, protecting the spinal canal and its contents—the spinal cord and nerve roots.
What Is a Laminectomy?
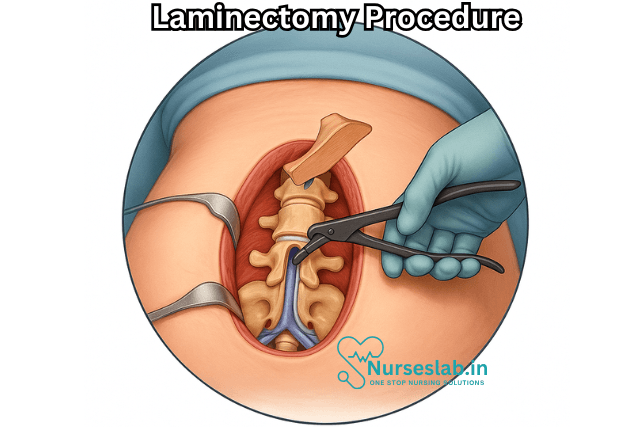
A laminectomy is the surgical removal of the lamina—the back part of the vertebral arch—which covers the spinal canal. By removing this bone, the surgeon creates more space within the spinal canal, thereby relieving abnormal pressure on the spinal cord or nerve roots. The procedure is also sometimes referred to as decompressive laminectomy.
Indications for Laminectomy
A laminectomy is most often recommended in the following situations:
- Spinal Stenosis: Narrowing of the spinal canal, often due to aging, arthritis, or degenerative changes, can compress the spinal cord and nerves, leading to pain, numbness, or weakness, especially in the legs.
- Herniated Disc: When a disc protrudes and compresses the nerve roots, a laminectomy may be performed in conjunction with discectomy to access and remove the herniated material.
- Spinal Tumors: Removal of lamina may be necessary to access and excise tumors impinging on neurological structures.
- Trauma: In cases involving spinal fractures or bone fragments, laminectomy can facilitate decompression and stabilization.
- Failed Conservative Treatment: Patients whose symptoms persist despite medications, physical therapy, and injections may benefit from surgical intervention.
Types of Laminectomy
There are several variations of the laminectomy procedure, tailored to the patient’s specific pathology and spinal region:
- Cervical Laminectomy: Performed on the neck (cervical) region of the spine.
- Thoracic Laminectomy: Targets the mid-back (thoracic) vertebrae.
- Lumbar Laminectomy: The most common type, performed on the lower back (lumbar spine).
- Laminotomy: Removal of only a portion of the lamina, preserving more of the spinal support structures.
- Minimally Invasive Laminectomy: Utilizes smaller incisions and specialized instruments, resulting in less tissue disruption and faster recovery.
Preoperative Preparation
Preparation for laminectomy involves a thorough evaluation to confirm the diagnosis and optimize patient health:
- Imaging studies such as MRI or CT scans to identify sites of compression.
- Physical and neurological assessment to document baseline function.
- Review of medical history, medications, allergies, and anesthetic risk.
- Preoperative instructions may include fasting, medication adjustments, and cessation of certain drugs (e.g., blood thinners).
Procedure Technique
The specifics of the laminectomy procedure may vary depending on the spinal level and underlying pathology, but typically include the following steps:
- Anaesthesia: The patient is usually placed under general anesthesia.
- Positioning: The patient lies face down on the operating table, with care taken to protect pressure points and maintain spinal alignment.
- Incision: A midline incision is made over the affected vertebrae.
- Muscle Dissection: Paraspinal muscles are gently retracted to expose the bony elements of the spine.
- Lamina Removal: The surgeon carefully removes the lamina with surgical instruments, taking care to avoid injury to the spinal cord or nerves.
- Decompression: Any bone spurs, disc Material, or other compressive tissue may be excised.
- Closure: The muscles and soft tissues are repositioned, and the incision is closed with sutures or staples.
Risks and Complications
As with any surgical procedure, laminectomy carries potential risks, including but not limited to:
- Infection at the surgical site
- Bleeding or hematoma formation
- Nerve injury leading to numbness, weakness, or paralysis (rare)
- Spinal fluid leak (dural tear)
- Blood clots in the legs (deep vein thrombosis)
- Persistent or recurrent symptoms
- Instability of the spine, sometimes necessitating fusion surgery
- Adverse reaction to anesthesia
Recovery After Laminectomy
Recovery times may vary based on the extent of surgery, patient health, and adherence to rehabilitation protocols. In general:
- Patients are usually up and walking the same day or the day after surgery.
- Hospital stay may range from a few hours (for minimally invasive procedures) to several days (for more extensive surgeries).
- Pain and stiffness are common initially, but improve with physical therapy and medications.
- Most people return to light activities within a few weeks, but strenuous activity and heavy lifting are typically restricted for several months.
- Physical therapy may be prescribed to restore flexibility, strength, and mobility.
- Regular follow-up visits are necessary to monitor healing and address complications, if any.
Expected Outcomes and Prognosis
Laminectomy is generally effective at relieving leg pain (sciatica) and neurological symptoms caused by nerve compression. Back pain relief can be variable, depending on preexisting spinal degeneration or other conditions. Most patients experience significant improvement in function and quality of life, but a small percentage may have persistent symptoms. Long-term outcomes are best when surgery is combined with lifestyle modifications, weight management, and appropriate exercise.
Alternatives to Laminectomy
Before recommending surgery, physicians often explore non-operative treatments, including:
- Physical therapy and exercise programs
- Medications such as anti-inflammatory drugs, pain relievers, and muscle relaxants
- Epidural steroid injections
- Chiropractic manipulation and alternative therapies
If these measures fail, and significant neurological impairment is present, surgical intervention is more strongly considered.
Advances in Laminectomy Technique
Recent advances include minimally invasive laminectomy, which utilizes endoscopic instruments and smaller incisions, reducing tissue trauma and promoting faster recovery. Image-guided navigation systems enhance surgical precision and safety. Some cases may be combined with spinal fusion to stabilize the spine if extensive bone removal is necessary.
Nursing Care of a Patient Undergoing Laminectomy Procedure
Laminectomy can significantly improve quality of life, but it is not without risks, and proper nursing care is essential to ensure the best possible outcomes for the patient.
Preoperative Nursing Care
Patient Assessment
- Medical History: Assess for comorbidities such as diabetes, hypertension, respiratory issues, and bleeding disorders that may affect perioperative management.
- Physical Examination: Focus on neurological status, including strength, sensation, reflexes, and pain levels.
- Baseline Vital Signs: Record baseline temperature, blood pressure, heart rate, respiratory rate, and oxygen saturation.
Patient Education and Psychological Preparation
- Explain the procedure, expected outcomes, and potential risks or complications to the patient and family.
- Address anxiety by allowing the patient to express fears and concerns, and provide reassurance.
- Educate about postoperative expectations, including restricted movement, pain management, and use of assistive devices.
- Discuss deep breathing, coughing, and leg exercises to prevent postoperative complications.
Preoperative Preparation
- Ensure all necessary investigations (blood tests, imaging, ECG) are completed.
- Obtain informed consent.
- Maintain NPO (nothing by mouth) status as per institutional guidelines.
- Prepare the surgical site by cleansing and shaving if required.
- Remove jewelry, dentures, nail polish, and contact lenses.
- Administer preoperative medications as ordered, including antibiotics or anxiolytics.
Immediate Postoperative Nursing Care
Initial Assessment
- Monitor airway, breathing, and circulation (the ABCs).
- Check vital signs every 15 minutes initially, gradually increasing the interval as the patient stabilizes.
- Observe for signs of respiratory distress, bleeding, or shock.
- Assess neurological status, including level of consciousness, limb movement, sensation, and pain.
Pain Management
- Administer prescribed analgesics promptly to control pain.
- Assess pain scale regularly and document responses to medications.
- Encourage non-pharmacological pain relief techniques, such as relaxation and distraction.
Positioning and Spinal Precautions
- Place the patient in a flat or slightly elevated position, depending on surgeon’s orders and institutional protocols.
- Maintain proper spinal alignment during turning or repositioning; use a log-roll technique to prevent torsion of the spine.
- Avoid pillows under the head or knees unless specifically ordered, as excessive flexion can compromise spinal alignment.
- Monitor for signs of edema or excessive drainage from the surgical site.
Monitoring for Complications
- Observe the surgical site for bleeding, hematoma, or signs of infection (redness, swelling, warmth, or purulent discharge).
- Monitor for cerebrospinal fluid (CSF) leakage, which may present as clear or yellowish drainage from the wound.
- Check for new or worsening neurological deficits: increased weakness, numbness, or loss of bowel/bladder control must be reported immediately.
- Assess for respiratory complications, including atelectasis and pneumonia, especially if the patient is reluctant to deep breathe due to pain.
Ongoing Postoperative Nursing Care
Neurological Monitoring
- Perform regular neurological assessments, comparing postoperative findings with preoperative baselines.
- Immediately report any changes, such as loss of sensation, movement, or incontinence.
- Document all neurological observations accurately and consistently.
Mobilization
- Encourage early, gradual mobilization as per the surgeon’s instructions to prevent complications such as deep vein thrombosis (DVT), pressure ulcers, and muscle wasting.
- Assist the patient into a sitting or standing position using the log-roll technique, maintaining spinal integrity.
- Provide ambulatory aids (e.g., walker or cane) if needed and ensure the patient is steady before walking.
- Educate about the importance of not twisting, bending, or lifting heavy objects until cleared by the healthcare team.
Wound Care
- Maintain a clean and dry surgical site.
- Change dressings as ordered using sterile technique to prevent infection.
- Inspect the incision regularly for signs of infection, dehiscence, or CSF leakage.
- Reinforce the importance of not scratching or disturbing the wound.
Prevention of Complications
- Encourage deep breathing and coughing exercises to prevent respiratory complications.
- Monitor for, and encourage, adequate hydration and nutrition to promote healing and bowel function.
- Administer prophylactic anticoagulants if prescribed, and use compression stockings or devices to reduce the risk of DVT.
- Encourage leg exercises and frequent position changes to enhance circulation and prevent pressure ulcers.
- Monitor bowel and bladder function; address constipation with stool softeners or laxatives as needed due to immobility and opioid use.
Patient and Family Education
- Teach wound care, signs of infection, and when to seek medical help.
- Instruct on activity restrictions: avoid heavy lifting, twisting, bending, and strenuous activity until cleared to do so.
- Discuss the importance of follow-up appointments and adherence to physical therapy regimens.
- Educate about pain management strategies and safe use of analgesics.
- Provide written instructions and clarify any uncertainties before discharge.
Psychosocial Support
- Assess the patient’s emotional and psychological status regularly.
- Provide reassurance and support to the patient and family to alleviate anxiety and promote coping.
- Refer to counseling or support groups if adjustment issues, depression, or anxiety are noted.
Discharge Planning and Home Care
Discharge Criteria
- Stable vital signs and neurologic status
- Ability to ambulate safely with or without assistance
- Effective pain control with oral medications
- Understanding of wound care and activity restrictions
- Support system available at home
Home Care Instructions
- Continue prescribed medications as directed.
- Maintain prescribed activity restrictions.
- Keep the surgical site clean and dry; attend follow-up visits for suture/staple removal as scheduled.
- Monitor for and report symptoms such as fever, increased pain, redness, swelling, or drainage at the incision.
- Gradually increase activity as tolerated, following the physical therapist’s recommendations.
- Contact the healthcare provider promptly if numbness, weakness, or problems with bowel/bladder control develop.
Common Complications and Their Management
- Infection: Prompt recognition and treatment with antibiotics; maintain sterile wound care practices.
- CSF Leak: Immediate reporting and evaluation; may require surgical intervention or specific wound management.
- Deep Vein Thrombosis: Early mobilization, pharmacological prophylaxis, and use of compression devices.
- Neurological Deficits: Immediate assessment and communication with the surgical team; may require imaging or revision surgery.
- Hematoma: Regular monitoring of the surgical site and prompt intervention if swelling or bleeding is detected.
REFERENCES
- American Academy of Orthopaedic Surgeons. Minimally Invasive Spine Surgery., https://orthoinfo.aaos.org/en/treatment/minimally-invasive-spine-surgery. Last reviewed 6/2022.
- American Academy of Orthopaedic Surgeons. Preparing for Low Back Surgery., https://orthoinfo.aaos.org/en/treatment/preparing-for-low-back-surgery/. Last reviewed 4/2022.
- American Academy of Physical Medicine and Rehabilitation. Post-laminectomy Pain., https://now.aapmr.org/post-laminectomy-pain/. Last reviewed 4/27/2022.
- Estefan M, Munakomi S, Camino Willhuber GO. Laminectomy. https://www.ncbi.nlm.nih.gov/books/NBK542274/). 2023 Aug 13. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-.
- Lundberg J and Langevin JP. Lumbar Microlaminectomy vs. Traditional Laminectomy., https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6370467. Fed Pract. 2017;34:32–5.
- MSD Manual. Video: Lumbar Laminectomy. https://www.msdmanuals.com/en-nz/home/multimedia/video/v14430136.
- National Library of Medicine (U.S.). Laminectomy. https://medlineplus.gov/ency/article/007389.htm. Last reviewed 12/12/2022.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


