


Last Updated on January 15, 2026 by Nurseslab.in Editorial Team
Introduction
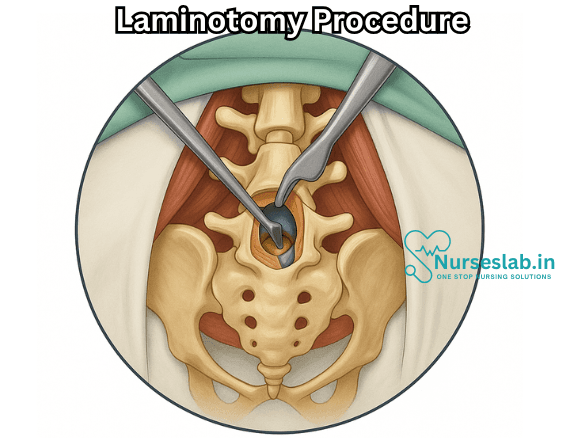
A laminotomy is a surgical procedure performed to relieve pressure on the spinal cord or spinal nerves by removing a portion of the lamina, a thin layer of bone that forms the back part of the vertebral arch. This operation is most commonly carried out to treat conditions such as spinal stenosis, herniated discs, or tumors that impinge upon neural elements. Unlike laminectomy, which involves removing the entire lamina, laminotomy is a less invasive alternative that preserves more of the spinal anatomy and stability.
Anatomy of the Spine
The human spine is composed of 33 vertebrae arranged in five regions: cervical, thoracic, lumbar, sacral, and coccygeal. Each vertebra has a body, a vertebral arch, and several processes. The lamina forms part of the vertebral arch, acting as a protective covering over the spinal cord and nerve roots. Attached to the lamina are muscles and ligaments that contribute to spinal stability and movement.
Indications for Laminotomy
Laminotomy is typically indicated for patients who suffer from conditions that result in narrowing of the spinal canal (spinal stenosis) or compression of the spinal nerves. The most common indications include:
- Spinal Stenosis: Narrowing of the spinal canal, often due to age-related degeneration, leading to nerve compression and symptoms such as pain, numbness, or weakness in the extremities.
- Herniated Disc: When a disc between the vertebrae bulges or ruptures, it can press on nearby nerves, causing pain or neurological symptoms.
- Spinal Tumors: Both benign and malignant growths can compress neural structures within the spinal canal.
- Congenital Disorders: Some individuals are born with spinal abnormalities that may require surgical decompression.
- Trauma: Injuries to the spine that result in bone fragments or swelling compressing the spinal cord or nerves.
Preoperative Assessment
Prior to surgery, a thorough assessment is conducted to identify the level and cause of nerve compression. This typically includes:
- Medical History and Physical Examination: The surgeon documents symptoms, duration, and any previous interventions.
- Imaging Studies: MRI (Magnetic Resonance Imaging) is most commonly used to visualize soft tissue structures, nerves, and the spinal cord. CT (Computed Tomography) and X-rays may also be used for detailed bone assessment.
- Neurological Evaluation: Assessing muscle strength, reflexes, and sensation to determine the extent of nerve involvement.
- Laboratory Tests: Blood work to evaluate general health and readiness for anesthesia.
The Laminotomy Procedure
Preparation
Before the procedure, patients are typically asked to fast for several hours. Preoperative antibiotics may be administered to reduce the risk of infection. The patient is positioned face-down (prone) on the operating table, and the area of the spine to be operated on is marked and sterilized.
Anesthesia
Laminotomy is most often performed under general anesthesia, although in some cases, regional anesthesia may be considered.
Incision
A small incision is made over the affected vertebral level. The length of the incision depends on the number of levels being treated and the patient’s anatomy.
Exposure
The muscles attached to the vertebrae are gently retracted to expose the lamina. Care is taken to minimize muscle damage and preserve spinal stability.
Bone Removal
A high-speed drill or surgical rongeur is used to remove a portion of the lamina, creating an opening (window) through which the surgeon can access the spinal canal. Only enough bone is removed to relieve the pressure on the compressed nerve roots or spinal cord.
Decompression
If necessary, additional tissue such as ligament or disc material that is causing compression may be removed. The main objective is to free the neural elements from any impingement.
Closure
Once decompression is complete, the surgical site is irrigated to reduce the risk of infection. The muscles and soft tissues are re-approximated, and the incision is closed in layers with sutures or staples.
Techniques and Variations
Laminotomy can be performed using traditional open surgery or minimally invasive techniques:
- Open Laminotomy: Involves a larger incision and more extensive muscle dissection but offers a broad view of the surgical site.
- Minimally Invasive Laminotomy: Uses smaller incisions and specialized instruments, often resulting in less tissue disruption, reduced blood loss, a shorter hospital stay, and faster recovery.
- Unilateral Laminotomy for Bilateral Decompression (ULBD): A minimally invasive variant where the surgeon operates from one side but decompresses both sides of the spinal canal.
Risks and Complications
As with any surgical procedure, laminotomy carries potential risks and complications, including:
- Infection: May occur at the incision site or deeper within the spine.
- Bleeding: Rare, but possible, especially in patients with bleeding disorders.
- Nerve Injury: Direct or indirect trauma to neural structures can result in numbness, weakness, or even paralysis (rare).
- Dural Tear: Accidental puncture of the membrane covering the spinal cord, potentially leading to cerebrospinal fluid leakage.
- Spinal Instability: Excessive bone removal may weaken the spine, sometimes necessitating fusion surgery.
- Persistent or Recurrent Symptoms: Some patients may not experience complete relief, or symptoms may return over time.
- Scar Tissue Formation: May cause future nerve irritation or compression.
Recovery and Rehabilitation
Recovery after laminotomy varies depending on the extent of surgery, the number of levels treated, and the patient’s overall health.
Immediately After Surgery
Patients are monitored in the recovery room for a few hours. Pain is managed with medications, and neurological status is checked frequently.
Hospital Stay
Most patients are discharged within 1 to 3 days if the surgery was uncomplicated. Minimally invasive procedures may allow for same-day discharge.
Rehabilitation
Physical therapy is often recommended to restore mobility, strengthen back muscles, and aid in a safe return to daily activities. Instructions are provided on how to move, sit, stand, and lift properly during the healing process.
Return to Work and Activities
Light activities and desk work can typically be resumed within 2 to 4 weeks, while more strenuous activities may require 6 to 12 weeks of recuperation. The timeline varies by individual.
Long-Term Prognosis
Most patients experience significant improvement in pain and neurological symptoms. However, the underlying cause of compression (such as degenerative disc disease) may progress, potentially requiring further treatment in the future.
Advantages of Laminotomy over Laminectomy
Laminotomy offers several benefits compared to the more extensive laminectomy:
- Tissue Preservation: Less bone and muscle are removed, maintaining greater spinal stability.
- Reduced Recovery Time: Patients typically heal faster due to the minimally invasive nature.
- Lower Risk of Postoperative Instability: By preserving more of the vertebral arch and supporting structures.
- Smaller Incisions: Leading to less scarring and decreased risk of infection.
Alternatives to Laminotomy
Depending on the severity and cause of spinal nerve compression, alternative treatments may be considered:
- Conservative Management: Physical therapy, medications, epidural steroid injections, and lifestyle modifications.
- Laminectomy: Removal of the entire lamina, usually reserved for severe or multi-level stenosis.
- Microdiscectomy: Specifically for herniated discs, involving removal of only the offending disc material.
- Foraminotomy: Widening the foramina (openings) where nerves exit the spinal canal.
- Spinal Fusion: Stabilizing adjacent vertebrae with bone graft and hardware, often used when instability is a concern.
Nursing Care of the Patient Undergoing Laminotomy Procedure
The procedure aims to ease pain, restore function, and improve the patient’s quality of life. As with any major spinal surgery, nursing care plays a critical role in ensuring optimal recovery, preventing complications, and supporting both the physical and emotional well-being of the patient.
Preoperative Nursing Care
Patient Assessment
- History and Physical Examination: Obtain a detailed medical history, including the duration and severity of symptoms, comorbid conditions, allergies, and previous surgeries.
- Diagnostic Evaluation: Review preoperative imaging (MRI, CT scan, X-rays) and laboratory results to identify potential risk factors.
- Pain Assessment: Document the character, location, intensity, and triggers of pain using appropriate pain scales.
- Psychological Evaluation: Assess anxiety, fear, and expectations related to surgery.
Patient Education
- Procedure Explanation: Educate the patient and family about the nature and purpose of laminotomy, expected outcomes, and potential risks.
- Preoperative Preparation: Instruct the patient on fasting, cessation of certain medications (e.g., anticoagulants), and skin cleansing protocols.
- Postoperative Expectations: Discuss the anticipated hospital stay, pain management plan, mobility restrictions, and use of assistive devices if needed.
Preoperative Preparations
- Consent: Ensure all informed consent documents are signed and properly filed.
- Preoperative Checklist: Complete the surgical safety checklist, confirming identity, surgical site, and procedure.
- IV Access and Medications: Establish intravenous access for fluids and medications. Administer preoperative antibiotics as ordered.
- Baseline Measurements: Record vital signs, neurological status, and assess the condition of the skin over the surgical site.
Intraoperative Nursing Care
Role in the Operating Room
- Sterile Technique: Maintain strict aseptic technique to prevent surgical site infections.
- Patient Positioning: Assist in proper positioning (usually prone or lateral) to ensure optimal surgical access and prevent pressure injuries.
- Monitoring: Continuously monitor vital signs, oxygen saturation, and neurological status during the procedure.
- Documentation: Accurately document intraoperative events, medications administered, and any complications.
Immediate Postoperative Nursing Care
Initial Assessment and Monitoring
- Airway and Breathing: Monitor airway patency, respiratory rate, and oxygen saturation. Provide supplemental oxygen as needed.
- Circulation: Assess heart rate, blood pressure, and peripheral perfusion. Watch for signs of bleeding or shock.
- Neurological Checks: Perform frequent neurological assessments, including motor strength, sensation, and movement of the lower extremities. Compare findings to preoperative baseline.
- Pain Management: Administer prescribed analgesics and evaluate their effectiveness. Use multimodal pain management strategies as appropriate.
- Fluid Balance: Monitor intake and output. Assess for signs of urinary retention or overhydration.
Potential Complications
- Hemorrhage: Watch for excessive drainage from the surgical site, hypotension, or tachycardia.
- Infection: Observe for fever, redness, swelling, or purulent discharge at the wound site.
- Neurological Deficits: Immediately report any new onset weakness, numbness, or loss of bowel/bladder control.
- Deep Vein Thrombosis (DVT): Monitor for signs of DVT such as swelling, redness, or pain in the calves.
- Respiratory Complications: Encourage deep breathing exercises and coughing to prevent atelectasis and pneumonia.
Wound and Drain Care
- Inspect the surgical dressing frequently for bleeding or excessive drainage.
- Maintain the integrity of the dressing; change as per protocol or if soiled.
- If drains are present, monitor output amount, color, and consistency; record findings and report abnormalities.
Early Mobilization
- Encourage movement as soon as medically permitted, often with physical therapy support.
- Assist the patient to sit on the edge of the bed, stand, or take short walks, as ordered.
- Use assistive devices (walker, cane) as required for stability and safety.
- Reposition the patient at least every two hours to prevent pressure ulcers.
Pain and Comfort Measures
- Administer pain medications as prescribed and assess relief regularly.
- Apply cold or warm compresses as appropriate to the surgical area for comfort.
- Promote relaxation techniques such as deep breathing, guided imagery, or music therapy.
Ongoing Postoperative Nursing Care
Neurological Monitoring
- Continue regular neurological assessments and compare with previous findings.
- Alert the surgical team to any changes, especially signs of spinal cord or nerve compromise.
Infection Prevention
- Maintain strict hand hygiene and aseptic technique during wound care.
- Monitor for and report early signs of infection.
- Encourage adequate nutrition and hydration to support healing and immunity.
Patient Education and Rehabilitation
- Teach the patient and family proper wound care techniques and the importance of adherence to follow-up appointments.
- Instruct on signs and symptoms that require immediate medical attention (e.g., increasing pain, fever, neurological changes).
- Provide guidance on activity restrictions, safe movement strategies, and the gradual resumption of daily activities.
- Collaborate with physical and occupational therapists to support the patient’s rehabilitation goals.
Psychosocial Support
- Offer emotional support and reassurance to address fears or anxiety about recovery and prognosis.
- Encourage involvement of family and friends in the care process.
- Refer to counseling or support groups if adjustment difficulties arise.
Discharge Planning
- Assess readiness for discharge based on mobility, pain control, wound healing, and the ability to perform self-care.
- Review prescribed medications, including analgesics, muscle relaxants, and antibiotics.
- Arrange for home health services or outpatient rehabilitation if needed.
- Provide clear, written discharge instructions and contact information for questions or emergencies.
Special Considerations
Care for Older Adults
- Monitor closely for delirium or cognitive changes, which may be more common in older patients postoperatively.
- Adapt mobility aids and home modifications to reduce the risk of falls.
Managing Chronic Conditions
- Coordinate care for comorbidities such as diabetes, hypertension, or cardiovascular disease.
- Monitor blood glucose and blood pressure regularly if indicated.
Pain Management Strategies
- Utilize a multimodal approach, combining non-opioid and opioid analgesics as appropriate.
- Incorporate non-pharmacological methods (e.g., repositioning, relaxation, ice/heat application).
- Educate on the risks of medication misuse and the importance of adhering to prescribed regimens.
Complication Prevention
- Encourage early mobilization and leg exercises to reduce the risk of DVT and pulmonary embolism.
- Promote incentive spirometry and breathing exercises to maintain respiratory function.
- Ensure adequate fluid intake and monitor for bowel or bladder dysfunctions.
- Be vigilant for signs of cerebrospinal fluid leak (e.g., clear drainage at wound site, headache when upright) and report them promptly.
REFERENCES
- American Academy of Orthopaedic Surgeons. Minimally Invasive Spine Surgery., https://orthoinfo.aaos.org/en/treatment/minimally-invasive-spine-surgery. Last reviewed 6/2022.
- American Academy of Orthopaedic Surgeons. Preparing for Low Back Surgery., https://orthoinfo.aaos.org/en/treatment/preparing-for-low-back-surgery/. Last reviewed 4/2022.
- Haddadi K, Ganjeh Qazvini HR. Outcome after Surgery of Lumbar Spinal Stenosis: A Randomized Comparison of Bilateral Laminotomy, Trumpet Laminectomy, and Conventional Laminectomy. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4824790/. Front Surg. 2016;3:19.
- National Health Services (U.K.). Lumbar Decompression Surgery, https://www.nhs.uk/conditions/lumbar-decompression-surgery/. Last reviewed 4/28/2022.
- Azar FM, et al. Degenerative disorders of the thoracic and lumbar spine. In: Campbell’s Operative Orthopaedics. 14th ed. Elsevier; 2021. https://www.clinicalkey.com.
- National Library of Medicine (U.S.). Laminectomy. https://medlineplus.gov/ency/article/007389.htm. Last reviewed 12/12/2022.
- Polikandriotis JA, Hudak EM, Perry MW. Minimally Invasive Surgery Through Endoscopic Laminotomy and Foraminotomy for the Treatment of Lumbar Spinal Stenosis. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3768246/. J Orthop. 2013;10(1):13-16.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


