


Last Updated on January 21, 2026 by Nurseslab.in Editorial Team
Supraglottoplasty is a surgical procedure primarily performed to treat laryngomalacia, the most common cause of stridor (noisy breathing) in infants and young children. The operation involves modifying or removing abnormal tissue above the vocal cords (the supraglottic region) to relieve airway obstruction and improve breathing. Supraglottoplasty has evolved as a minimally invasive, highly effective intervention that significantly improves airway patency and quality of life for affected patients.
What is Supraglottoplasty?
Supraglottoplasty is an endoscopic airway surgery that targets the supraglottic structures, which include the epiglottis, aryepiglottic folds, arytenoids, and sometimes the false vocal cords. These structures can be abnormally floppy or redundant in conditions like laryngomalacia, leading to partial or complete collapse of the airway during inspiration. The goal of supraglottoplasty is to remove or reshape these tissues to prevent airway collapse and reduce symptoms such as stridor, feeding difficulties, and obstructive sleep apnea.
Indications for Supraglottoplasty
The most common indication for supraglottoplasty is moderate to severe laryngomalacia that does not improve with conservative treatment. Laryngomalacia typically presents in infancy and is characterized by inspiratory stridor, feeding problems, failure to thrive, and, in severe cases, cyanotic episodes.
Other indications may include:
- Recurrent aspiration due to supraglottic collapse
- Obstructive sleep apnea related to supraglottic tissue prolapse
- Persistent respiratory distress despite conservative management
- Severe gastroesophageal reflux exacerbating airway obstruction
Most cases of laryngomalacia are mild and resolve spontaneously by 18–24 months of age. Surgery is reserved for those whose symptoms compromise breathing and nutrition or pose a risk to life.
Preoperative Evaluation
A thorough assessment is crucial before deciding on supraglottoplasty. The evaluation often includes:
- Detailed medical history and physical examination
- Flexible laryngoscopy to directly visualize the airway and identify the sites and patterns of collapse
- Assessment for synchronous airway lesions (other anomalies along the airway)
- Evaluation for associated comorbidities, such as neurological impairment or cardiac disease
- Feeding and swallowing assessment
In selected cases, additional tests such as sleep studies (polysomnography), pH monitoring for reflux, or imaging studies may be warranted.
Anatomy of the Supraglottis
The supraglottic region sits just above the true vocal cords and comprises several important structures:
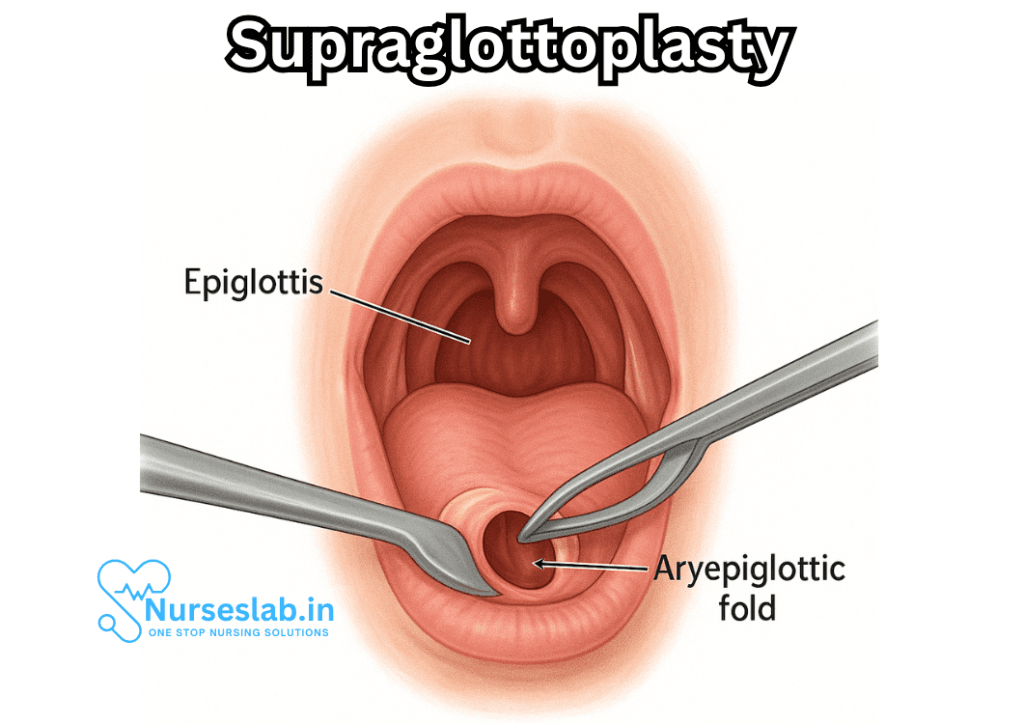
- The epiglottis: a leaf-shaped flap of cartilage that protects the airway during swallowing
- Aryepiglottic folds: mucosal bands stretching from the epiglottis to the arytenoid cartilages
- Arytenoid cartilages: paired cartilages that help open and close the vocal cords
- False vocal cords (vestibular folds): tissues that sit just above the true vocal cords
In laryngomalacia, these tissues may be excessively pliable, redundant, or malformed, leading to airway collapse.
The Supraglottoplasty Procedure
Supraglottoplasty is typically performed under general anesthesia using endoscopic techniques, which allow for visualization and intervention through the mouth without external incisions.
The key steps in the procedure include:
- Patient positioning and administration of general anesthesia
- Insertion of a laryngoscope to visualize the supraglottic structures
- Assessment of the dynamic airway collapse and identification of the offending tissues
- Precise removal, incision, or reshaping of redundant aryepiglottic folds, trimming of the epiglottis if necessary, and sometimes excision of redundant tissue on the arytenoids or false vocal cords
- Use of specialized instruments such as microscissors, microdebriders, lasers (e.g., CO2 laser), or radiofrequency devices for tissue removal
- Meticulous hemostasis to control bleeding
- Postoperative suctioning and assessment to ensure adequate airway patency
The procedure is tailored to the child’s unique anatomy and the severity of airway collapse. The use of endoscopic techniques allows for less trauma, faster recovery, and minimal scarring.
Types of Supraglottoplasty
Different techniques can be employed based on the specific pathology:
- Aryepiglottic Fold Division: Incising or excising the aryepiglottic folds to prevent inward collapse
- Epiglottectomy: Partial removal or reshaping of the epiglottis if it is large or floppy
- Arytenoid Reduction: Removal of redundant mucosa over the arytenoid cartilages
- Combined Procedures: Often, a combination of these techniques is necessary for optimal results
Postoperative Care and Recovery
After surgery, patients are closely monitored in a hospital setting for respiratory complications, bleeding, or swelling. Most children experience significant improvement in breathing within hours to days.
Postoperative considerations include:
- Observation for airway edema or laryngospasm
- Pain management and hydration
- Gradual reintroduction of oral feeding
- Speech and swallowing therapy if indicated
- Follow-up laryngoscopy to assess healing and airway patency
Hospital stays are usually brief, ranging from a few hours to a couple of days, depending on the severity of disease and the presence of other health problems.
Outcomes and Prognosis
Supraglottoplasty is highly effective, with success rates reported between 80–95% in resolving airway obstruction and improving symptoms. Most children experience rapid improvement in stridor, feeding ability, and sleep quality. In a minority of cases, additional surgeries may be required due to persistent or recurrent airway symptoms.
Potential complications include:
- Airway edema and stridor
- Aspiration or feeding difficulties
- Formation of supraglottic scar tissue (webbing or stenosis)
- Need for repeat surgery
- Rarely, tracheostomy if severe airway compromise occurs
Long-term outcomes are generally excellent, especially in otherwise healthy children without significant comorbidities.
Risks and Complications
While supraglottoplasty is considered safe, as with any surgical intervention, risks exist:
- Bleeding during or after the procedure
- Infection
- Excessive removal of tissue leading to airway instability or aspiration
- Recurrence of symptoms if not enough tissue is removed
- Need for further surgeries
Careful surgical planning and technique minimize these risks. Postoperative swelling is managed with steroids and observation.
Special Considerations
Supraglottoplasty may be less effective or riskier in children with:
- Syndromic conditions or craniofacial abnormalities
- Neurological impairment affecting airway tone
- Multiple synchronous airway lesions
A multidisciplinary approach, involving pediatric otolaryngologists, anesthesiologists, pulmonologists, gastroenterologists, and speech therapists, ensures the best outcomes for complex cases.
Alternatives to Surgery
Not all cases of laryngomalacia or supraglottic obstruction require surgical management. Mild symptoms often respond to conservative measures such as:
- Positioning modifications during feeding
- Thickening of feeds to reduce aspiration
- Treatment of associated gastroesophageal reflux with medications
- Observation and supportive care
Surgery is reserved for those who fail conservative therapy or who have life-threatening symptoms.
History and Evolution of Supraglottoplasty
Originally, tracheostomy was the only surgical option for severe laryngomalacia, but it carried significant risks and complications. The development of endoscopic supraglottoplasty in the late 20th century revolutionized pediatric airway management. Advances in surgical instruments, anesthesia, and perioperative care have made the procedure safer and more effective.
Patient and Family Education
Families should be counseled about the nature of laryngomalacia, the expected course of disease, the risks and benefits of surgery, and the likelihood of improved breathing and feeding postoperatively. Education about signs of airway distress and when to seek urgent help is essential for optimal outcomes.
Nursing Care of Patients Undergoing Supraglottoplasty
Nursing care for patients undergoing supraglottoplasty is critical in ensuring optimal outcomes, minimizing complications, and providing essential support throughout the perioperative and postoperative periods. This document offers a detailed guide to the nursing management of these patients, encompassing preparation, monitoring, intervention, and family education.
1. Preoperative Nursing Care
1.1. Patient Assessment
- Comprehensive History: Assess the patient for respiratory distress, feeding difficulties, stridor, cyanosis, apnea, and history of recurrent respiratory infections.
- Physical Examination: Evaluate airway patency, respiratory rate, ease of breathing, use of accessory muscles, and oxygen saturation. Note any signs of failure to thrive, dehydration, or retractions.
- Diagnostic Preparation: Ensure relevant investigations are completed, such as flexible laryngoscopy, chest X-ray, and blood tests (CBC, coagulation profile, etc.).
- Allergy & Medication Review: Document allergies and current medications, especially anticoagulants, as these may need to be withheld prior to surgery.
1.2. Patient and Family Education
- Explain the procedure in age-appropriate language, emphasizing the reasons for surgery and expected outcomes.
- Discuss the perioperative process, including fasting requirements, anesthesia plan, and anticipated monitoring.
- Provide information on postoperative expectations such as voice changes, sore throat, potential for respiratory support, and length of hospital stay.
- Offer emotional support and address concerns or misconceptions.
1.3. Preoperative Preparation
- Ensure NPO (nothing by mouth) status as per anesthesia guidelines to prevent aspiration risks.
- Establish IV access for medication administration and hydration.
- Confirm informed consent has been obtained and documented.
- Prepare emergency airway management equipment and suction apparatus in the operating room and recovery area.
2. Intraoperative Nursing Responsibilities
2.1. Safety and Monitoring
- Assist with patient positioning, typically supine with neck slightly extended for optimal airway visualization.
- Monitor vital signs continuously, paying special attention to oxygen saturation and end-tidal CO₂ if available.
- Maintain sterility in the operating field and support the surgical team as needed with instruments and supplies.
- Be prepared to assist in emergent airway interventions, such as bag-mask ventilation or tracheostomy, if complications arise.
2.2. Communication
- Update the surgical and anesthesia team regarding any changes in the patient’s baseline condition.
- Ensure accurate documentation of all intraoperative events.
3. Postoperative Nursing Care
3.1. Airway Management
- Continuous Monitoring: Observe the patient closely for signs of airway compromise, including increased stridor, retractions, tachypnea, cyanosis, or decreased oxygen saturation.
- Positioning: Maintain the child in a semi-Fowler’s or upright position to facilitate airway patency and reduce edema.
- Humidified Oxygen: Administer humidified oxygen as prescribed to reduce airway irritation and promote mucosal healing.
- Suctioning: Perform gentle oral or nasopharyngeal suctioning as needed to clear secretions, being careful to avoid trauma to the surgical site.
- Emergency Preparedness: Keep emergency airway equipment (e.g., bag-valve-mask, laryngoscope, endotracheal tubes, tracheostomy set) at the bedside.
3.2. Pain and Comfort Management
- Assess for pain using age-appropriate scales (e.g., FLACC for infants, Wong-Baker FACES for older children).
- Administer analgesics as prescribed, considering non-opioid options (e.g., acetaminophen, ibuprofen) to avoid respiratory depression.
- Provide comfort measures such as cuddling, distraction techniques, and a quiet environment.
3.3. Monitoring for Complications
- Respiratory Distress: Watch for worsening stridor, retractions, or episodes of apnea, and notify the medical team immediately if they occur.
- Bleeding: Observe for signs of bleeding from the mouth or nose, increased swallowing, or vomiting of blood. Report promptly and be prepared to intervene.
- Laryngeal Edema: Look for progressive hoarseness, muffled voice, difficulty swallowing, or signs of airway obstruction. Administer prescribed steroids if indicated to reduce swelling.
- Infection: Monitor temperature, incision site (if external), and overall clinical status. Report any signs of infection to the medical team.
3.4. Fluid and Nutritional Support
- Ensure adequate hydration, initially via IV fluids if necessary, then gradual reintroduction of oral intake as tolerated.
- Begin with clear fluids and advance diet based on tolerance and absence of aspiration risk.
- Encourage small, frequent feeds, maintaining upright positioning during and after feeds to prevent aspiration.
- Monitor for signs of dehydration, such as dry mucous membranes, decreased urine output, and lethargy.
3.5. Communication and Education
- Educate parents or caregivers regarding signs of potential complications post-discharge (e.g., respiratory distress, bleeding, fever).
- Demonstrate safe feeding techniques and positioning for infants and young children.
- Provide written instructions and emergency contact information for urgent concerns.
- Offer reassurance and support as families transition to home care.
4. Discharge Planning and Follow-Up
4.1. Criteria for Discharge
- Stable airway with no evidence of respiratory distress.
- Adequate pain control with oral medications.
- Ability to tolerate oral fluids and nutrition without aspiration.
- No active bleeding or signs of infection.
- Caregivers are confident and competent in recognizing complications and providing care.
4.2. Follow-Up Care
- Schedule follow-up appointments with otolaryngology and primary care for ongoing assessment and monitoring.
- Encourage continued observation for delayed onset airway symptoms or feeding issues.
- Support participation in speech or feeding therapy if recommended due to ongoing difficulties.
5. Special Considerations
5.1. Care of High-Risk Patients
Some patients—such as those with neurologic impairments, syndromic features, or severe laryngomalacia—may have increased risk for complications and require extended monitoring or intensive care admission postoperatively. Nurses should maintain heightened vigilance, collaborate with multidisciplinary teams, and anticipate more prolonged recovery needs.
5.2. Psychosocial Support
Surgery can be distressing for both patients and families. Nurses play a vital role in assessing anxiety, offering comfort, and connecting families with resources such as counseling, social work, or peer support groups.
5.3. Documentation
Careful and accurate documentation is essential to ensure continuity of care and legal protection. Record all assessments, interventions, patient responses, teaching, and communication with the healthcare team.
REFERENCES
- Kang ES, Turkdogan S, Yeung JC. Disposition to pediatric intensive care unit post supraglottoplasty repair: a systematic review. https://pubmed.ncbi.nlm.nih.gov/37106398/. J Otolaryngol Head Neck Surg. 2023 Apr 27;52(1):35.
- Maksimoski M, Li C. Surgical Management of Pediatric Obstructive Sleep Apnea Beyond T&A – Tongue Base and Larynx. https://pubmed.ncbi.nlm.nih.gov/38538515/ Otolaryngol Clin North Am. 2024 Mar 26:S0030-6665(24)00034-3.
- Del Do M, Song SA, Nesbitt NB, Spaw MC, Chang ET, Liming BJ, Cable BB, Camacho M. Supraglottoplasty surgery types 1-3: A practical classification system for laryngomalacia surgery. Int J Pediatr Otorhinolaryngol. 2018 Aug;111:69-74. https://pubmed.ncbi.nlm.nih.gov/29958617/
- Morse E, Pereira N, Liu K, Veler H, Maresh A. Management and outcomes of obstructive sleep apnea in infants. https://pubmed.ncbi.nlm.nih.gov/37075592/. Int J Pediatr Otorhinolaryngol. 2023 May;168:111558.
- Pu S, Xu H, Li X. Supraglottoplasty in neonates and infants: A radiofrequency ablation approach. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5839815/. Medicine (Baltimore). 2018 Feb;97(7):e9850.
- van der Heijden M, Dikkers FG, Halmos GB. Treatment outcome of supraglottoplasty vs. wait-and-see policy in patients with laryngomalacia. Eur Arch Otorhinolaryngol. 2016 Jun;273(6):1507-13. doi: 10.1007/s00405-016-3943-3. Epub 2016 Feb 29. PMID: 26924742; PMCID: PMC4858546.
- van der Heijden M, Dikkers FG, Halmos GB. Treatment outcome of supraglottoplasty vs. wait-and-see policy in patients with laryngomalacia. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4858546/ Eur Arch Otorhinolaryngol. 2016 Jun;273(6):1507-13.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


