


Trabeculectomy is a surgical procedure primarily used to manage and treat glaucoma, a group of eye conditions characterized by increased intraocular pressure (IOP) that can lead to optic nerve damage and potential vision loss. As one of the most common and time-tested surgical interventions for glaucoma, trabeculectomy plays a critical role in preserving vision when medical or less invasive approaches prove insufficient. This document provides a comprehensive exploration of trabeculectomy, covering its indications, surgical techniques, patient selection criteria, benefits, risks, postoperative care, and long-term outcomes.
Understanding Glaucoma and the Need for Surgical Intervention
Glaucoma is often described as the “silent thief of sight” because it typically progresses without noticeable symptoms until significant vision loss has occurred. Elevated intraocular pressure is the most important modifiable risk factor in the progression of glaucomatous optic neuropathy. While eye drops, oral medications, and laser therapies are the first lines of treatment to control IOP, there are cases where these options do not achieve the desired pressure reduction or are poorly tolerated due to side effects or compliance issues. In such scenarios, surgical intervention is considered, with trabeculectomy being a gold standard for decades.
What is Trabeculectomy?
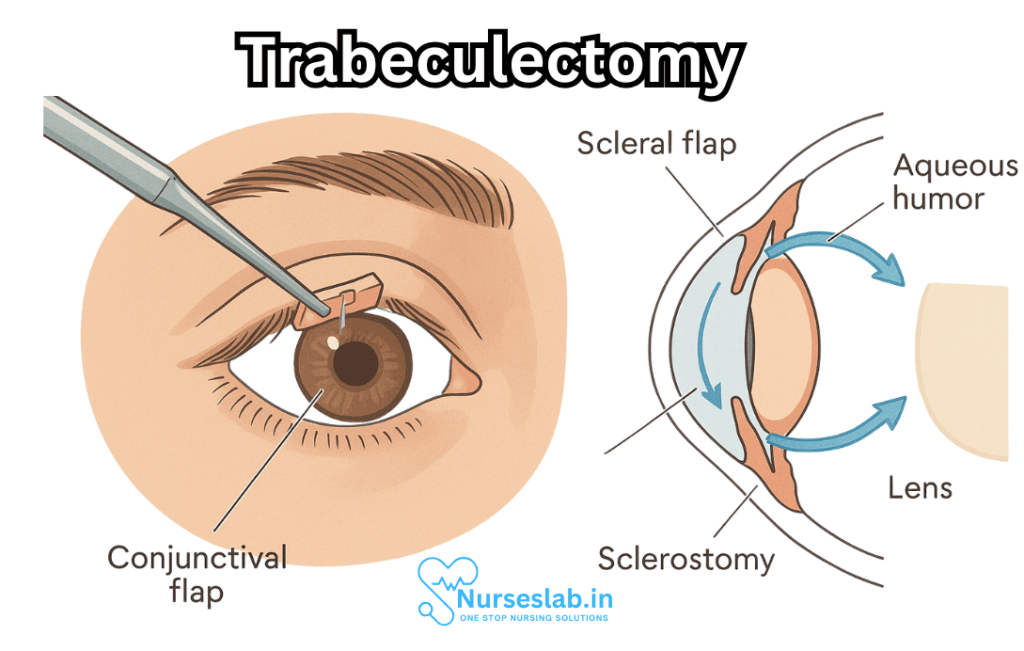
Trabeculectomy is a filtration surgery designed to create a new drainage pathway for the aqueous humor—the clear fluid that fills the front part of the eye. By facilitating the drainage of this fluid from the anterior chamber to the space beneath the conjunctiva (the thin membrane covering the white of the eye), the procedure lowers intraocular pressure and reduces the risk of further optic nerve damage.
Historical Perspective
Developed in the late 1960s, trabeculectomy replaced earlier and less effective surgical procedures. Its success and adaptability have made it the cornerstone of surgical glaucoma management worldwide, although new techniques and devices are continually being developed.
Indications for Trabeculectomy
The main indication for trabeculectomy is the diagnosis of glaucoma—most commonly open-angle glaucoma—that is not adequately controlled with medications and/or laser procedures. Other indications include:
- Primary open-angle glaucoma unresponsive to medical therapy
- Angle-closure glaucoma, especially after failed laser iridotomy
- Secondary glaucomas, such as neovascular, uveitic, or congenital glaucoma
- Patients unable to tolerate medications due to side effects or allergy
- Progressive optic nerve damage or visual field loss despite optimal non-surgical management
The Trabeculectomy Procedure
Although the surgical steps may vary based on individual patient characteristics and surgeon preference, the core principles remain consistent.
Preoperative Evaluation
A thorough preoperative assessment is vital and includes:
- Comprehensive eye examination and documentation of optic nerve status
- Measurement of intraocular pressure and visual field testing
- Assessment of the conjunctiva for suitability for filtration surgery
- Review of systemic health and current medications
Patients are counseled about the risks, benefits, potential alternatives, and the importance of postoperative care.
Surgical Technique
The procedure is typically performed under local anesthesia, sometimes with sedation. General anesthesia may be used for children or anxious adults.
- A small section of the conjunctiva is opened, often in the upper part of the eye, to access the sclera (white of the eye).
- A partial thickness scleral flap is created and dissected to form a door-like structure.
- An opening is made under this flap into the anterior chamber, providing an exit for the aqueous humor.
- A small piece of trabecular meshwork and underlying tissue is removed to form the new drainage pathway.
- The scleral flap is closed loosely with sutures to control the rate of fluid flow.
- The conjunctiva is then meticulously closed to prevent leaks.
- Often, anti-fibrotic agents such as mitomycin C or 5-fluorouracil are applied to reduce scarring and improve long-term patency of the drainage pathway.
At the conclusion of the surgery, a filtering “bleb” forms under the conjunctiva where the aqueous humor accumulates before being absorbed by surrounding tissues.
Postoperative Care and Follow-up
Recovery after trabeculectomy requires close monitoring to ensure the filtering bleb functions properly and to manage potential complications. Postoperative care includes:
- Frequent eye examinations, especially during the first few weeks after surgery
- Use of topical antibiotics and corticosteroids to prevent infection and suppress inflammation
- Adjustment of sutures, if necessary, to optimize fluid drainage
- Avoiding strenuous activity, eye rubbing, and exposure to contaminants
Patients are also educated about the signs of infection, excessive discomfort, or changes in vision that warrant immediate medical attention.
Benefits of Trabeculectomy
The primary benefit of trabeculectomy is the effective and sustained reduction of intraocular pressure, which can slow or halt the progression of glaucoma and thus preserve remaining vision. Other benefits include:
- Long-term IOP control with a single surgery in many cases
- Reduction or elimination of the need for glaucoma medications
- Potentially improved quality of life for patients with advanced or poorly controlled glaucoma
Risks and Complications
As with any surgical procedure, trabeculectomy carries risks. Complications can be immediate or delayed and may include:
- Hypotony (excessively low eye pressure)
- Bleb failure due to scarring
- Infection of the bleb (blebitis) or deep eye infections (endophthalmitis)
- Cataract formation or acceleration of pre-existing cataracts
- Choroidal effusion or hemorrhage
- Loss of vision in rare cases
Proper surgical technique, careful patient selection, and diligent postoperative monitoring reduce the likelihood and impact of these complications.
Long-term Outcomes and Prognosis
Trabeculectomy has a favorable long-term success rate, with many patients achieving significant intraocular pressure reduction for years after surgery. The longevity of the filtering bleb and the absence of serious complications are key determinants of success. Advances in surgical technique and anti-scarring measures continue to enhance outcomes.
Who is a Good Candidate?
Candidates for trabeculectomy are typically patients with moderate to advanced glaucoma who have not achieved adequate IOP control with medications or laser therapies, or who cannot safely use these treatments. The decision to proceed with surgery is based on individual risk profiles, vision needs, and life expectancy.
Alternatives and Adjuncts to Trabeculectomy
While trabeculectomy remains a cornerstone, newer surgical approaches and minimally invasive glaucoma surgeries (MIGS) have expanded the treatment landscape:
- Glaucoma drainage devices (tubes and shunts)
- Laser trabeculoplasty
- Non-penetrating filtering surgeries (deep sclerectomy, viscocanalostomy)
- Various MIGS procedures (iStent, Xen Gel Stent, etc.)
Nursing Care of Patients After Trabeculectomy
Effective nursing care following trabeculectomy is critical for optimizing surgical outcomes, ensuring patient safety, and promoting recovery. This comprehensive guide discusses the essential aspects of nursing care for patients post-trabeculectomy, highlighting assessment, monitoring, patient education, complication management, and emotional support.
Preoperative Nursing Care
Patient Assessment and Preparation
- Baseline Assessment: Evaluate the patient’s medical history, medication use, allergies, visual acuity, and history of glaucoma progression. Document baseline IOP and optic nerve status.
- Education: Explain the surgical procedure, anticipated outcomes, and potential risks. Address patient anxieties and provide reassurance.
- Medication Review: Confirm preoperative instructions regarding discontinuation or continuation of certain medications, such as anticoagulants.
- Infection Prevention: Ensure preoperative administration of prescribed topical antibiotics.
- Consent: Verify informed consent has been obtained and documented.
Immediate Postoperative Nursing Care
Patient Monitoring and Safety
- Vital Signs: Monitor vital signs, including blood pressure and pulse, as systemic changes can affect ocular perfusion.
- Ocular Assessment: Assess the operated eye for pain, redness, swelling, bleeding, and discharge. Check dressing and shield placement.
- Positioning: Encourage the patient to rest in a semi-Fowler’s position to reduce intraocular pressure. Advise avoidance of lying flat, which may increase ocular congestion.
- Pain Management: Administer prescribed analgesics and provide comfort measures. Assess and document pain intensity, location, and character.
- Antiemetic Administration: Prevent nausea and vomiting, which may increase intraocular pressure and risk of hemorrhage.
- Medication Administration: Administer postoperative eyedrops, including antibiotics and steroids, as ordered. Ensure aseptic technique during instillation to prevent infection.
Ongoing Postoperative Care
Monitoring for Complications
- Signs of Infection: Observe for redness, swelling, discharge, or fever. Report any abnormal findings promptly. Emphasize strict hand hygiene.
- Bleeding or Hyphema: Monitor for blood in the anterior chamber or on the eye surface. Report excessive bleeding immediately.
- Leakage From Bleb: Inspect for excessive aqueous humor leakage around the surgical site (bleb), which can lead to hypotony or infection.
- Choroidal Detachment: Watch for signs of pain, decreased vision, or abnormal fundus findings, and notify the ophthalmology team if suspected.
- Elevated or Reduced IOP: Monitor IOP as scheduled. Both excessively high and low IOP may threaten surgical success and vision.
- Vision Changes: Assess and report any sudden decrease in visual acuity, blurred vision, or loss of vision.
Eye Protection and Care
- Eye Shield: Encourage use of an eye shield, especially during sleep, to protect the operated eye from accidental trauma.
- Dressings: Maintain clean, dry dressings. Change as per protocol using sterile technique.
- Hygiene: Advise against touching or rubbing the eye. Teach proper handwashing technique before administering eyedrops or caring for the eye.
Patient Education and Counseling
Medication Compliance
- Eyedrop Administration: Educate the patient and caregivers on correct administration technique, adherence to dosing schedule, and storage of medications.
- Medication Side Effects: Discuss possible side effects, such as irritation or allergic reactions, and advise when to seek medical attention.
Activity Restrictions
- Physical Exertion: Advise against heavy lifting, straining, bending over, or vigorous exercise for several weeks postoperatively.
- Bathing and Hygiene: Instruct the patient to avoid water entering the operated eye during bathing. Use a clean washcloth to gently clean the face.
- Returning to Work: Discuss a gradual return to work and daily activities, depending on recovery and occupational demands.
Follow-Up Appointments
- Regular Monitoring: Stress the importance of scheduled follow-up visits for IOP measurement, wound assessment, and overall eye health.
- Reporting Symptoms: Educate on warning signs such as pain, redness, discharge, vision changes, or swelling, and encourage prompt reporting.
Psychosocial Support
- Anxiety and Adjustment: Provide emotional support to help patients cope with vision changes, dependence during recovery, and fear of complications.
- Family Involvement: Encourage family members to assist with care, medication administration, and emotional encouragement.
- Resources: Provide information about support groups for patients with glaucoma and vision impairment.
Discharge Planning
Home Care Instructions
- Medication: Review the medication regimen with the patient and family, ensuring clear understanding of names, dosages, and times.
- Eye Shield: Reinforce the importance of wearing the eye shield as directed.
- Environmental Safety: Recommend creating a safe home environment to prevent falls or accidental eye trauma.
- Emergency Contacts: Provide contact information for the ophthalmologist, clinic, and emergency services.
Common Complications and Nursing Management
Infection (Endophthalmitis)
- Assessment: Observe for increasing pain, redness, swelling, or purulent discharge.
- Intervention: Notify healthcare provider promptly and prepare for possible diagnostic evaluation or additional therapy.
Hypotony (Low Intraocular Pressure)
- Assessment: Monitor for excessive leakage from bleb, shallow anterior chamber, or choroidal detachment.
- Intervention: Collaborate with ophthalmology for potential surgical revision or other interventions.
Failure of Filtration (High Intraocular Pressure)
- Assessment: Routine IOP measurements, patient symptoms (headache, eye pain).
- Intervention: Assist with additional procedures such as needling or anti-fibrotic medications if necessary.
Bleb Leak
- Assessment: Inspect for excessive fluid leakage and signs of infection.
- Intervention: Report findings and support preparation for surgical repair or revision.
Documentation
- Record all assessments, findings, interventions, patient responses, and education provided.
- Maintain detailed records of medication administration, IOP measurements, wound care, and follow-up recommendations.
REFERENCES
- American Academy of Ophthalmology EyeWiki. Glaucoma Drainage Devices. https://eyewiki.aao.org/Glaucoma_Drainage_Devices. Updated 8/9/2024.
- Khandelwal RR, et al. (2015). Surgical outcomeof safe surgery system trabeculectomy combined with cataract extraction. DOI:
https://doi.org/10.1038/eye.2014.294 - American College of Ophthalmology EyeWiki. Trabeculectomy. https://eyewiki.aao.org/Trabeculectomy. Updated 3/21/2023.
- BrightFocus Foundation. Glaucoma Surgery Series: Trabeculectomy. https://www.brightfocus.org/glaucoma/article/glaucoma-surgery-series-trabeculectomy. Published 7/7/2021.
- Dietze J, Blair K, Zeppieri M, Havens SJ. Glaucoma. https://www.ncbi.nlm.nih.gov/books/NBK538217/. 2024 Mar 16. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
- Gurnani B, Tripathy K. Minimally Invasive Glaucoma Surgery. https://www.ncbi.nlm.nih.gov/books/NBK582156/. 2023 Aug 25. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
- Ma AK, Lee JH, Warren JL, Teng CC. GlaucoMap – Distribution of Glaucoma Surgical Procedures in the United States. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7473985/. Clin Ophthalmol. 2020 Aug;14:2551-2560.
- Prineas S. Local and Regional Anesthesia for Ophthalmic Surgery. In: Hadzic A. eds. Hadzic’s Textbook of Regional Anesthesia and Acute Pain Management. 2nd ed. McGraw-Hill Education; 2017.
- Salmon JF. Glaucoma. In: Riordan-Eva P, Augsburger JJ, eds. Vaughan & Asbury’s General Ophthalmology. 19th ed. McGraw-Hill Education; 2017.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


