


Introduction
Ventriculostomy is a critical neurosurgical procedure that involves creating an opening into the ventricular system of the brain, typically to drain cerebrospinal fluid (CSF), relieve intracranial pressure (ICP), or access the ventricular space for diagnostic or therapeutic purposes. Most commonly performed as an external ventricular drain (EVD), ventriculostomy remains a cornerstone in the management of a range of acute neurosurgical conditions, including traumatic brain injury, subarachnoid hemorrhage, hydrocephalus, and intracranial infections.
Anatomy and Physiology of the Ventricular System
The human brain contains a complex network of cavities known as the ventricular system, which is filled with cerebrospinal fluid. The system comprises four primary ventricles:
- Lateral Ventricles (right and left): The largest and most accessible, located within the cerebral hemispheres.
- Third Ventricle: Situated in the midline between the thalami.
- Fourth Ventricle: Located dorsal to the pons and upper medulla.
CSF circulates through this system, providing cushioning, waste removal, and nutrient delivery to the brain and spinal cord. Blockages or disruptions to CSF flow can cause dangerous increases in intracranial pressure, damaging neural tissue.
Indications for Ventriculostomy
Ventriculostomy is utilized in a variety of clinical scenarios, including but not limited to:
- Acute hydrocephalus: Obstruction of CSF pathways, often due to hemorrhage, tumor, infection, or congenital malformation.
- Traumatic brain injury (TBI): Monitoring and management of raised ICP, especially when there is parenchymal swelling or bleeding.
- Subarachnoid hemorrhage (SAH): To manage hydrocephalus secondary to blood obstructing CSF flow or to monitor ICP.
- Infectious conditions: Such as ventriculitis or meningitis, when CSF sampling or drainage is indicated.
- Intraventricular hemorrhage: Especially in neonates, to remove blood and relieve pressure.
- Measurement of ICP: In patients with severe brain injury or suspicion of elevated ICP.
- Administration of intraventricular medications: Such as antibiotics or chemotherapeutic agents.
Types of Ventriculostomy
Ventriculostomy may be classified into several types based on the method and intended duration:
- External Ventricular Drainage (EVD): A temporary system for draining CSF externally, most common in acute neurosurgical settings.
- Ventriculoperitoneal (VP) Shunt: A permanent diversion of CSF from the ventricles to the peritoneal cavity.
- Endoscopic Third Ventriculostomy (ETV): A minimally invasive procedure to create an opening in the floor of the third ventricle, usually for obstructive hydrocephalus.
Preoperative Considerations
Prior to ventriculostomy, thorough assessment is essential:
- Review imaging studies (CT/MRI) to assess ventricular size, location, and underlying pathology.
- Evaluate coagulation status and correct any abnormalities to minimize bleeding risk.
- Informed consent, explaining risks, benefits, and alternatives to the patient or family.
- Preparation of equipment and sterile field.
Technical Aspects of the Procedure
The most common technique, EVD, is typically performed at the bedside or in the operating room under sterile conditions. The steps generally include:
- Patient positioning: The patient is placed supine with the head slightly elevated and stabilized.
- Landmark identification: The entry point is typically at Kocher’s point—2–3 cm lateral to the midline and 1 cm anterior to the coronal suture.
- Preparation and draping: The scalp is shaved and disinfected, and local anesthesia is administered.
- Burr hole creation: A small hole is drilled through the skull at the chosen entry site.
- Dural opening: The dura mater is incised with a scalpel.
- Catheter insertion: A soft ventricular catheter is gently advanced toward the lateral ventricle, confirmed by free flow of CSF.
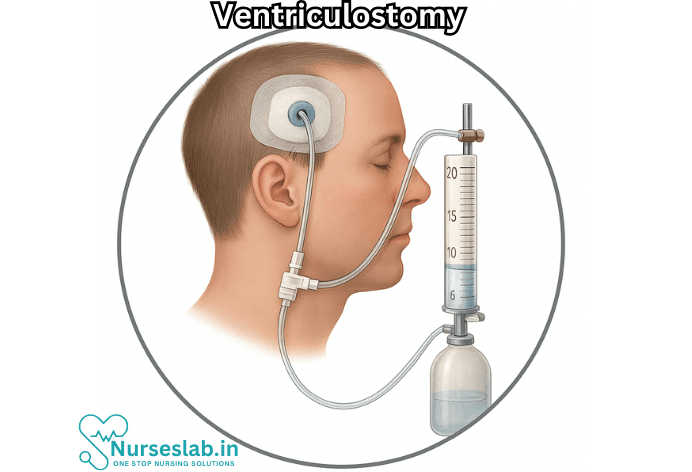
- Catheter securing: The catheter is sutured to the scalp and connected to an external drainage and monitoring system.
- Dressing: The site is covered with a sterile dressing, and the external system is secured and set at a predefined height to regulate drainage.
Monitoring and Management
Once in place, the EVD serves both therapeutic and diagnostic roles. Key aspects of management include:
- ICP Monitoring: The system allows continuous measurement of intracranial pressure, with normal values typically ranging from 7–15 mmHg in adults.
- CSF Drainage: The amount, color, and character of the CSF are monitored; sudden changes may indicate infection or blockage.
- Infection Prevention: Strict aseptic technique reduces the risk of catheter-associated infections.
- Neurological Assessment: Frequent exams are conducted to monitor for changes in consciousness or new deficits.
- System Maintenance: The system must be checked regularly for occlusion, leaks, or accidental dislodgement.
Complications
Although ventriculostomy is often lifesaving, it is not without risks. Some of the main complications include:
- Infection: Ventriculostomy-related infections, such as ventriculitis or meningitis, are among the most serious complications, with reported rates from 5–20%.
- Hemorrhage: Insertion can cause bleeding in the brain or along the catheter tract.
- Catheter malposition: Misplacement can render the device non-functional or cause neurological injury.
- Blockage or occlusion: Blood clots or debris may obstruct CSF flow through the catheter.
- Overdrainage: Excessive CSF drainage can lead to subdural hematoma or collapse of the ventricles.
- CSF leakage: At the exit site, increasing infection risk.
Postoperative Care and Removal
Careful monitoring continues after placement. The EVD is typically removed once the underlying condition is resolved or has stabilized. Removal must be performed under sterile conditions, and the site is closely observed for signs of infection or CSF leak. In cases of persistent hydrocephalus, conversion to a permanent CSF diversion procedure (such as a VP shunt) may be necessary.
Recent Advances and Future Directions
The field of ventriculostomy continues to evolve:
- Image-guided placement: Use of neuronavigation and ultrasound for more precise catheter placement.
- Antibiotic-impregnated catheters: Technology to reduce infection risk.
- Miniaturized and telemetric ICP monitoring devices: For less invasive and more accurate long-term monitoring.
- Simulation-based training: Enhancing neurosurgical skills for safer and more effective procedures.
Nursing Care of a Patient with Ventriculostomy
The procedure carries significant risks, and meticulous nursing care is essential to ensure patient safety, accurate monitoring, and prevention of complications.
Nursing Assessment
Baseline Assessment:
- Perform a comprehensive neurological assessment including Glasgow Coma Scale, pupil size and reactivity, motor response, and level of consciousness.
- Document vital signs: blood pressure, heart rate, respiratory rate, temperature, and oxygen saturation.
- Assess for signs of increased ICP (e.g. headache, vomiting, altered mental status, papilledema).
- Examine the ventriculostomy site for bleeding, swelling, or signs of infection.
Ongoing Monitoring:
- Perform regular neurological checks as per the unit protocol (typically hourly or more frequently if indicated).
- Monitor and document ICP readings and waveform patterns.
- Record CSF drainage amount, color, and clarity on a strict flow sheet.
- Observe for changes in the patient’s neurological status, which may indicate worsening ICP or complications.
Care of the Ventriculostomy System
- Ensure all connections are secure and the system is properly leveled at the reference point, usually the tragus of the ear, to ensure accurate pressure readings.
- Maintain the system as a closed circuit whenever possible to minimize infection risk.
- Do not allow air to enter the system; air bubbles can interfere with readings and increase infection risk.
- Avoid unnecessary manipulation of the catheter or drainage system.
- Label all ports and lines clearly.
Preventing and Managing Complications
Infection
- Practice strict aseptic technique during any handling of the catheter, dressing changes, or CSF sampling.
- Change dressings as per hospital policy using sterile technique. Typically, this is done every 24-48 hours or sooner if soiled.
- Monitor for signs of infection: fever, erythema, discharge at insertion site, changes in CSF appearance.
- Send CSF samples for culture if infection is suspected.
- Educate family and visitors about not touching the system.
Hemorrhage
- Observe for sudden neurological deterioration, which may signal bleeding.
- Monitor insertion site for hematoma or excessive bleeding.
- Report any abnormal findings promptly to the neurosurgical team.
Obstruction
- Check for a decrease in CSF drainage and rising ICP readings, which may indicate catheter blockage.
- Inspect tubing for kinks or clots.
- Do not attempt to flush the catheter unless specifically instructed by medical staff.
- Notify the provider immediately if obstruction is suspected.
Overdrainage
- Monitor the level of the drainage system relative to the patient’s head; too low can lead to excessive CSF drainage and complications such as subdural hematoma.
- Be alert for signs of overdrainage: headache, altered consciousness, or focal neurological deficits.
- Adjust the drainage system height only under physician orders.
Patient and Family Education
- Explain the purpose and functioning of the ventriculostomy to the patient (if possible) and family.
- Discuss the importance of not moving or pulling on the catheter or tubing.
- Educate regarding signs and symptoms of infection and increased ICP.
- Provide information about activity restrictions, such as avoiding sudden movements or changing head position without nurse assistance.
Documentation
- Record all ICP measurements, CSF drainage amounts, and changes in patient condition.
- Document dressing changes, site assessments, interventions, and communications with the medical team.
- Chart education provided to the patient and family.
Collaborative Management
- Work closely with neurosurgeons and intensivists to manage drainage parameters and respond to changes in patient status.
- Coordinate with infection control to monitor infection risk and trends.
- Communicate promptly about any concerns such as system malfunction, abnormal CSF findings, or neurological deterioration.
Special Nursing Considerations
- Maintain appropriate sedation and analgesia as ordered, balancing neurological assessment needs with patient comfort.
- Assess for complications related to immobility, such as pressure injuries and deep vein thrombosis.
- Monitor fluid balance and electrolytes, as excessive CSF drainage can impact overall homeostasis.
- Support the patient’s psychosocial needs, acknowledging the anxiety and fear that can accompany neurological procedures.
Removal and Post-Removal Care
- Prepare for removal as per physician orders, ensuring all equipment is available and sterile procedures are maintained.
- Monitor closely for neurological changes and signs of CSF leak or infection after catheter removal.
- Continue site care and educate the patient about symptoms that require immediate reporting, such as fever, headache, or fluid leakage.
REFERENCES
- Deopujari CE, Karmarkar VS, Shaikh ST. Endoscopic Third Ventriculostomy: Success and Failure. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5426452/. J Korean Neurosurg Soc. 2017 May;60(3):306-314.
- Munakomi S, Das JM. Ventriculostomy. [Updated 2023 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK545317/
- Hydrocephalus Association (U.S.). What to Expect With ETV Surgery. https://www.hydroassoc.org/etv-surgery/. Last reviewed 2021..
- Munakomi S, M Das J. Ventriculostomy. https://www.ncbi.nlm.nih.gov/books/NBK545317/. [Updated 2023 Aug 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-.
- National Health Services (U.K.). Hydrocephalus Treatment. https://www.nhs.uk/conditions/hydrocephalus/treatment/. Last reviewed 2/6/2023.
- Wisinger D, Mest-Beck L. Ventriculostomy: a guide to nursing management. J Neurosci Nurs. 1990 Dec;22(6):365-9. doi: 10.1097/01376517-199012000-00006. PMID: 2148765.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


