


Last Updated on January 10, 2026 by Nurseslab.in Editorial Team
Introduction
Neurolysis is a medical procedure aimed at the deliberate destruction or disruption of nerve tissue to relieve pain, restore function, or reduce spasticity. This intervention is employed in various clinical settings, from the management of chronic pain syndromes to the treatment of spasticity in neurological disorders. The term “neurolysis” is derived from the Greek words “neuron” (nerve) and “lysis” (loosening or destruction), reflecting its fundamental principle: the targeted dissolution or interruption of nerve activity.
Historical Background
The concept of neurolysis dates back to the late 19th and early 20th centuries, when pioneering clinicians sought methods to alleviate intractable pain, particularly in cancer patients. Early techniques relied on surgical removal or interruption of nerves. With advances in medical technology, chemical and thermal methods were developed, making the procedure safer and more effective. Today, neurolysis is a cornerstone in pain management and rehabilitation medicine, with ongoing research expanding its indications and efficacy.
Types of Neurolysis
Neurolysis can be classified based on the method of nerve destruction, the target nerves, and the clinical intent. The two primary types are:
- Chemical Neurolysis: Involves the injection of neurolytic agents (such as alcohol, phenol, or glycerol) to chemically destroy nerve fibers.
- Thermal Neurolysis: Utilizes heat (radiofrequency ablation, cryotherapy, or laser) to physically disrupt nerve conduction.
Additionally, neurolysis may be described as temporary (nerve block with anesthetic agents) or permanent (irreversible destruction of nerve tissue).
Chemical Neurolysis
Chemical neurolysis is commonly used for the management of chronic pain, particularly in cancer patients and those with severe, refractory pain syndromes. Agents such as ethanol (alcohol) and phenol are injected near or into nerves, leading to denaturation of proteins, necrosis, and Wallerian degeneration of nerve fibers. The effect is a long-lasting interruption of pain signals.
Thermal Neurolysis
Thermal neurolysis involves the use of heat or cold to disrupt nerve function. Techniques such as radiofrequency ablation (RFA) deliver controlled heat via a needle electrode, causing coagulation necrosis of the targeted nerve. Cryoablation, in contrast, uses extreme cold to achieve similar results. Laser neurolysis employs focused light energy to destroy nerve tissue.
Other Techniques
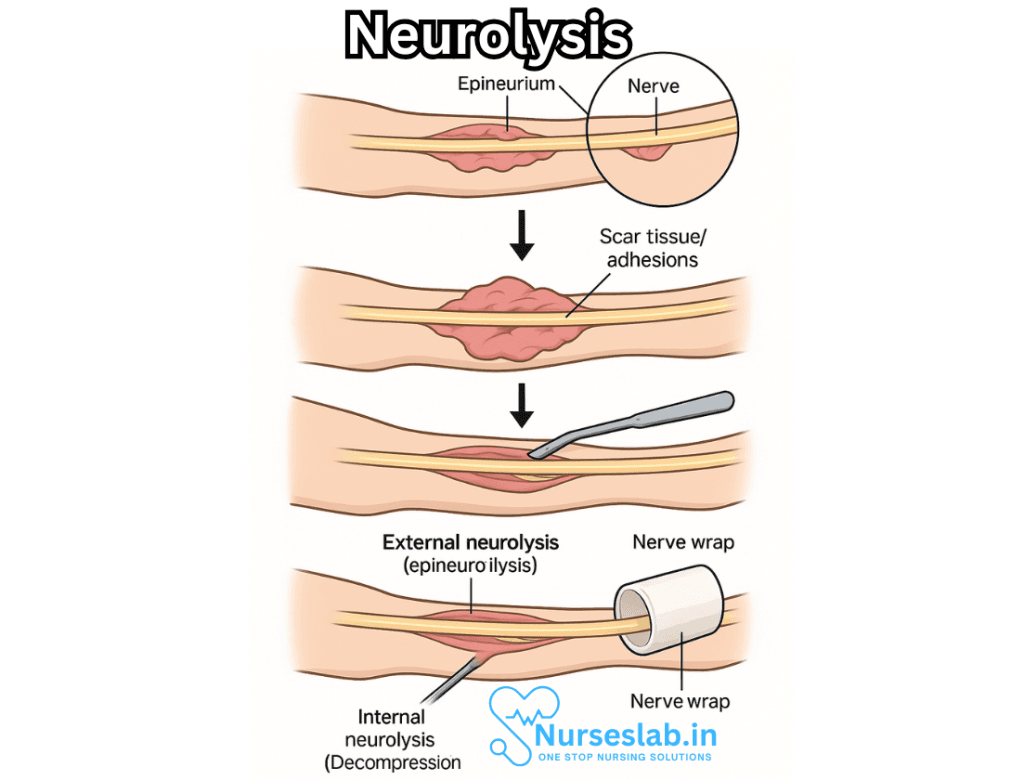
Surgical neurolysis entails the physical removal or decompression of nerves. It can also refer to the process of freeing a nerve from scar tissue (neurolytic neuroplasty), as seen in cases of nerve entrapment or post-traumatic adhesions.
Indications and Clinical Applications
Neurolysis is indicated in a wide array of clinical scenarios. The most common include:
- Pain Management: Severe, intractable pain, especially in malignancy (e.g., pancreatic cancer, pelvic cancers).
- Spasticity Management: In patients with upper motor neuron lesions (e.g., stroke, cerebral palsy, multiple sclerosis), neurolysis can relieve debilitating spasticity by targeting hyperactive motor nerves.
- Nerve Entrapment Syndromes: Neurolysis may be used surgically to release nerves from adhesions or compressive structures.
- Peripheral Neuropathies: Selective neurolysis can help alleviate pain or dysfunction in certain neuropathic conditions.
Common Procedures
- Celiac Plexus Neurolysis: Used for relief of intractable abdominal pain in upper gastrointestinal cancers; involves injection of neurolytic agents near the celiac plexus.
- Stellate Ganglion Neurolysis: Performed for sympathetically mediated pain syndromes of the upper limb or face.
- Sciatic Nerve Neurolysis: Can be used surgically or chemically for selected cases of severe sciatic pain or entrapment.
- Phenol or Alcohol Blocks: Used for spasticity management in rehabilitation medicine, often targeting obturator, femoral, or sciatic nerves.
Techniques and Procedure
The approach to neurolysis varies depending on the target nerve, patient condition, and the chosen modality. However, the general steps include:
- Patient Assessment: Thorough evaluation of the patient’s history, physical examination, and diagnostic imaging (ultrasound, CT, fluoroscopy) to identify the target nerve(s).
- Anesthesia: Local anesthesia is commonly used; sedation or general anesthesia may be required in select cases.
- Needle Placement: Image-guided placement of the needle or probe to ensure accurate targeting of the nerve.
- Test Block: A test injection of local anesthetic may be performed to confirm appropriate nerve targeting and to predict likely outcome.
- Neurolytic Agent Delivery: Injection of chemical agent, or application of thermal energy as per the selected technique.
- Monitoring and Recovery: Observation for immediate adverse effects and post-procedure follow-up for long-term outcomes.
Benefits and Outcomes
Neurolysis can provide significant relief from chronic pain and spasticity, frequently improving the quality of life for patients with debilitating symptoms. The outcomes depend on the underlying condition, technique, and patient factors:
- Pain relief is often substantial and long-lasting, particularly in cancer-related pain syndromes.
- Improved mobility and function in patients with severe spasticity.
- Reduction in the need for systemic pain medications, thus lowering the risk of side effects and dependency.
However, the benefits must be weighed against potential risks and complications, and patient selection is critical to optimize outcomes.
Risks and Complications
Like any medical procedure, neurolysis carries potential risks, which may include:
- Nerve Injury: Unintended damage to adjacent nerves, leading to sensory or motor deficits.
- Infection: Introduction of pathogens at the injection or surgical site.
- Bleeding or Hematoma: Particularly in patients with coagulopathies or when vascular structures are nearby.
- Transient or Permanent Numbness: Loss of sensation in the area supplied by the treated nerve.
- Muscle Weakness or Paralysis: If motor nerves are affected.
- Allergic Reactions: To the neurolytic agents or anesthetics used.
- Post-procedure Pain: Sometimes pain may worsen temporarily before improving.
Careful technique, image guidance, and thorough pre-procedure evaluation minimize these risks.
Contraindications
Neurolysis is not suitable for all patients. Contraindications include:
- Local or systemic infection.
- Coagulopathy or bleeding disorders.
- Allergy to neurolytic agents or anesthetics.
- Poorly defined pain syndromes where the target nerve cannot be reliably identified.
- Unrealistic patient expectations or inability to participate in follow-up care.
Recent Advances and Future Directions
Recent years have seen significant advances in neurolytic techniques, particularly with the advent of minimally invasive, image-guided procedures. Ultrasound, CT, and MRI guidance have enhanced the precision and safety of nerve targeting. Additionally, developments in radiofrequency and cryoablation technologies have expanded the indications for neurolysis while reducing complications.
Research is ongoing into novel neurolytic agents, refined delivery methods, and the integration of neurolysis within multidisciplinary pain management and rehabilitation programs. There is increasing interest in patient-reported outcomes, quality-of-life measures, and individualized care pathways, ensuring that neurolysis is tailored to the unique needs of each patient.
Ethical and Practical Considerations
The decision to undertake neurolysis must be based on a careful consideration of potential benefits, risks, and patient preferences. In palliative care, neurolysis can provide invaluable relief for patients with end-stage disease, enabling greater comfort and dignity. However, irreversible nerve destruction must be approached with caution in patients with non-terminal conditions, as it carries the risk of permanent sensory or motor loss.
Effective communication and informed consent are vital, ensuring that patients and families understand the goals, potential outcomes, and limitations of neurolysis.
Nursing Care of Patients Undergoing Neurolysis
This Nursing Care provides an in-depth overview of nursing responsibilities and best practices when caring for patients who have undergone neurolysis, fostering optimal recovery, minimising complications, and supporting holistic wellbeing.
Preoperative Assessment and Preparation
- Comprehensive Patient Evaluation: Assess the patient’s baseline neurological status, pain patterns, and overall health. Obtain a thorough history of pain management strategies, medication usage, allergies, and psychosocial factors.
- Education and Consent: Explain the neurolysis procedure, expected outcomes, possible risks, and alternatives. Facilitate informed consent through clear communication, addressing any patient or family concerns.
- Preparation for Procedure: Ensure preoperative investigations (e.g., imaging studies, blood work) are completed and reviewed. Collaborate with the medical team to optimise pain control and anxiety reduction prior to intervention.
- Psychosocial Support: Recognise the emotional impact of chronic pain and impending intervention, providing reassurance and psychological support.
Immediate Post-Procedural Care
- Monitoring and Assessment: Closely monitor vital signs, level of consciousness, pain intensity, and neurological function. Watch for changes in motor or sensory status, as neurolysis can alter nerve function acutely.
- Pain Management: Evaluate the effectiveness of neurolysis in controlling pain. Adjust analgesic regimens as needed, considering the possible reduction in pain medication requirements. Monitor for new types of pain, such as deafferentation pain or neuropathic symptoms.
- Complication Surveillance: Be vigilant for procedure-related complications, including infection, bleeding, nerve injury, or unintended loss of function. Assess for signs of autonomic dysfunction (e.g., hypotension, changes in sweating), particularly when neurolysis involves sympathetic nerves.
- Wound and Site Care: If a surgical approach was used, inspect the site for signs of infection, hematoma, or delayed healing. Maintain sterile technique in dressing changes.
- Early Mobilisation: Encourage gentle mobilisation as tolerated, preventing complications such as deep vein thrombosis, pressure injuries, and pulmonary issues. Collaborate with physiotherapists to ensure safe movement.
Ongoing Assessment and Support
- Neurological Surveillance: Regularly assess sensory and motor function in the affected region(s), documenting changes meticulously. Use validated pain scales and neurological checklists to track progress.
- Pain Reassessment: Continue to monitor pain levels, adjusting management strategies in response to the patient’s evolving symptoms. Address any concerns about residual or breakthrough pain, using multimodal approaches where appropriate.
- Physical Function and Rehabilitation: Support patients in regaining strength and function, particularly if neurolysis has resulted in temporary or permanent deficits. Coordinate with rehabilitation specialists for tailored exercise and reconditioning programs.
- Prevention of Secondary Complications: Implement strategies to reduce the risk of infection, skin breakdown, aspiration (if cranial nerves are involved), and other secondary complications. Encourage deep breathing exercises and proper nutrition.
- Medication Management: Review all medications for interactions and side effects, especially when neurolysis affects autonomic or somatic nerves. Ensure patients understand changes in their medication regimen post-procedure.
Patient Education and Empowerment
- Recognising Complications: Teach patients to identify warning signs such as increasing pain, new sensory or motor deficits, fever, swelling, or wound changes. Emphasise the importance of prompt reporting to healthcare providers.
- Self-Care Strategies: Educate about lifestyle adjustments, positioning techniques, and protective measures to avoid injury in areas with reduced sensation or strength. Advise on skin care and fall prevention.
- Medication Adherence: Stress the importance of taking prescribed medications as directed, including analgesics and adjunct therapies. Discuss potential side effects and when to seek medical attention.
- Activity Guidance: Provide recommendations on safe levels of activity, gradual increase in mobility, and participation in rehabilitation programs. Set realistic goals for recovery in collaboration with the patient and family.
- Follow-Up Scheduling: Arrange regular follow-up visits for ongoing monitoring, adjustment of care plans, and timely intervention for emerging issues.
Holistic and Psychosocial Care
- Emotional Wellbeing: Acknowledge the psychological burden of chronic pain and invasive procedures. Offer support through empathetic listening, counselling referrals, and encouragement of participation in support groups.
- Family and Caregiver Involvement: Include significant others in education, care planning, and decision-making when appropriate, while respecting patient autonomy and confidentiality.
- Cultural Sensitivity: Respect the cultural beliefs and preferences of the patient and family in all aspects of care, from pain management to dietary choices and emotional support.
- Spiritual Care: Facilitate access to spiritual resources if desired, supporting the patient’s coping mechanisms and sense of meaning.
Interdisciplinary Collaboration
- Team Communication: Work closely with physicians, pain specialists, physiotherapists, occupational therapists, pharmacists, and social workers to coordinate comprehensive care.
- Continuous Evaluation: Participate in regular team meetings to review progress, update care plans, and address any barriers to recovery.
- Advocacy: Champion the patient’s needs and preferences within the healthcare system, ensuring timely access to resources and interventions.
REFERENCES
- D’Souza RS, Hooten WM. Neurolytic Blocks. https://www.ncbi.nlm.nih.gov/books/NBK537360/. 2023 Jan 29. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-
- Tariq RA, Mueller M, Green MS. Neuraxial Neurolysis. [Updated 2023 May 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537157/
- Escaldi S. Neurolysis: A Brief Review for a Fading Art. https://pubmed.ncbi.nlm.nih.gov/30626512/. Phys Med Rehabil Clin N Am. 2018 Aug;29(3):519-527.
- Jones RC 3rd, Lawson E, Backonja M. Managing Neuropathic Pain. Med Clin North Am. 2016 Jan;100(1):151-167.
- Sachdev AH, Gress FG. Celiac Plexus Block and Neurolysis: A Review. https://pubmed.ncbi.nlm.nih.gov/30241645/. Gastrointest Endosc Clin N Am. 2018 Oct;28(4):579-586.
- Gupta M, Abdallah RT, Abd-Elsayed A, Chakravarthy K, Day M, Deer T, Diwan S, Knezevic NN, Mehta ND, Schatman ME, Soin A, Staats P. A Review of Nonsurgical Neurolytic Procedures for Neuropathic Pain. J Pain Res. 2025 Feb 25;18:879-895.
- Wu R, Majdalany BS, Lilly M, Prologo JD, Kokabi N. Agents Used for Nerve Blocks and Neurolysis. https://pubmed.ncbi.nlm.nih.gov/36406019/. Semin Intervent Radiol. 2022 Nov;39(4):387-393.
- Wu R, Majdalany BS, Lilly M, Prologo JD, Kokabi N. Agents Used for Nerve Blocks and Neurolysis. Semin Intervent Radiol. 2022 Nov 17;39(4):387-393.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


