


Understanding Yttrium-90 Radioembolization for Liver Cancer and Beyond
Introduction
Yttrium-90 (Y-90) treatment, also known as Y-90 radioembolization or selective internal radiation therapy (SIRT), is an advanced form of internal radiation therapy primarily used in the management of liver cancers. Leveraging the unique physical properties of the radioactive isotope yttrium-90, this technique delivers targeted radiation directly to tumors while minimizing exposure to the surrounding healthy tissue. Over the past two decades, Y-90 treatment has emerged as a powerful tool in the fight against primary liver tumors such as hepatocellular carcinoma (HCC) and secondary (metastatic) liver malignancies, especially those arising from colorectal cancer.
What is Y-90 Treatment?
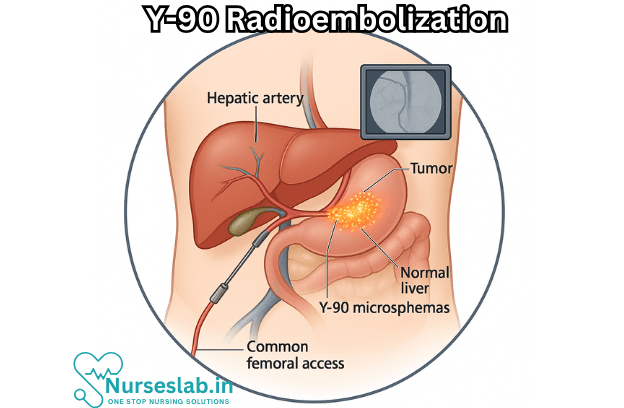
At its core, Y-90 radioembolization is a minimally invasive procedure that combines the principles of radiation therapy and embolization. The treatment involves the administration of millions of tiny beads, called microspheres, that are impregnated with the radioactive isotope yttrium-90. These microspheres are delivered directly into the arteries that supply blood to the liver tumors. Once in place, they emit high-energy beta radiation, selectively destroying cancer cells while sparing much of the surrounding healthy liver tissue.
How Y-90 Works
Unlike external beam radiation therapy, which delivers radiation from outside the body, Y-90 therapy is a form of brachytherapy (internal radiation). The microspheres are typically made of either glass or resin, each type with specific properties, and are engineered to become lodged within the tumor’s blood vessels. The beta particles emitted by yttrium-90 travel only a short distance—typically just a few millimeters—ensuring that the majority of the radiation is confined to the tumor itself. Over a span of about two weeks, the radioactive activity of Y-90 decays, delivering a substantial dose of therapy with minimal impact on the rest of the liver or the body.
Indications for Y-90 Treatment
Y-90 radioembolization is most commonly indicated for patients with:
- Unresectable hepatocellular carcinoma (HCC), where surgery is not an option due to tumor location, multifocality, or patient comorbidities.
- Liver-dominant metastatic cancer, especially metastases from colorectal cancer, neuroendocrine tumors, and other primaries that preferentially spread to the liver.
- Patients who have failed or are not candidates for other local therapies like transarterial chemoembolization (TACE) or ablative techniques.
- Bridge to liver transplantation, to control tumor growth while awaiting a donor organ.
The Y-90 Treatment Process
The process typically unfolds in several stages:
1. Evaluation and Planning
Each case begins with a multidisciplinary evaluation, involving oncologists, interventional radiologists, hepatologists, and sometimes surgeons. The team will review imaging studies such as CT or MRI scans to assess the size, number, and location of tumors. Blood tests are performed to evaluate liver and kidney function, and to ensure the patient is a suitable candidate.
A key step in planning is the mapping angiogram, where the arteries supplying the liver and the tumors are studied using contrast dye. During this procedure, the interventional radiologist also identifies any blood vessels that may carry microspheres away from the liver (potentially causing non-target radiation to organs like the stomach or lungs) and blocks them off as needed.
2. Simulation with Technetium-99m Macroaggregated Albumin (MAA)
Before the actual Y-90 treatment, a test injection with a radioactive tracer (Tc-99m MAA) is performed. This simulates the flow of Y-90 microspheres and allows the team to estimate how much of the dose might go to the lungs or other non-target organs. A nuclear medicine scan then helps ensure the treatment will be both safe and effective.
3. The Y-90 Infusion Procedure
On the day of treatment, the patient is typically given mild sedation and local anesthesia. A catheter is inserted through the femoral or radial artery and navigated into the hepatic arteries feeding the tumor. The Y-90 microspheres are then slowly infused. The procedure usually takes 60 to 90 minutes and is performed on an outpatient basis.
4. Post-Treatment Monitoring
After the procedure, patients are monitored for a few hours and can usually return home the same day. Follow-up imaging is scheduled weeks later to assess the treatment’s effectiveness and check for any side effects.
Benefits of Y-90 Radioembolization
- Targeted Therapy: Delivers high doses of radiation directly to tumors, sparing much of the normal liver tissue.
- Minimally Invasive: Unlike surgery, no large incisions are required, leading to faster recovery.
- Outpatient Procedure: Most patients return home the same day.
- Suitability for Advanced Disease: Can be used even when tumors are large, multifocal, or close to critical structures.
- Combination with Other Therapies: Can be integrated with systemic chemotherapy, immunotherapy, or used as a bridge to transplantation.
Risks and Side Effects
While Y-90 treatment is generally well-tolerated, it is not without risks. Potential side effects include:
- Post-Embolization Syndrome: A group of symptoms, including fatigue, low-grade fever, abdominal pain, and nausea, can occur in the days following treatment.
- Liver Dysfunction: Rarely, the radiation can damage healthy liver tissue, leading to a decline in liver function.
- Gastrointestinal Ulcers: If microspheres inadvertently reach the stomach or intestines, ulcers or bleeding may develop.
- Radiation Pneumonitis: Very rarely, radiation reaching the lungs can cause inflammation.
- Other Risks: Infection, bleeding, or damage to blood vessels at the catheter insertion site.
Outcomes and Effectiveness
Numerous studies have demonstrated the efficacy of Y-90 radioembolization in shrinking liver tumors, improving symptoms, and in some cases, extending survival. The degree of response depends on factors such as the type of tumor, the extent of liver involvement, and the patient’s overall health. In selected patients, Y-90 can downstage tumors to make them eligible for surgical resection or transplantation.
Response rates for primary liver cancer can reach up to 80%, with partial or complete tumor shrinkage seen in many patients. For metastatic colorectal cancer, Y-90 has been shown to control liver disease even after failure of standard chemotherapy.
Life After Y-90 Treatment
Most patients experience a recovery period of several days to a week, during which symptoms of post-embolization syndrome may occur. Routine follow-up includes imaging, laboratory tests, and clinic visits to monitor liver function and treatment response. While some patients may need additional therapies, others can enjoy prolonged periods of disease control.
Nursing Care of Patients Undergoing Yttrium-90 (Y-90) Treatment
Nurses play a crucial role in the multidisciplinary team managing patients receiving Y-90 therapy. Their responsibilities span from pre-procedural assessment and education to post-procedure care and monitoring for complications.
Pre-Procedure Nursing Care
Patient Education
- Explanation of Procedure: Provide the patient and their family with detailed information about Y-90 treatment, including the rationale, benefits, potential risks, and expected outcomes. Use language appropriate to the patient’s level of understanding.
- Pre-Procedural Requirements: Instruct the patient on fasting requirements, medication adjustments (e.g., withholding anticoagulants), and the need for laboratory tests such as liver function, coagulation profile, and renal function.
- Discussion of Side Effects: Review potential side effects, such as fatigue, abdominal pain, nausea, mild fever, and, rarely, radiation-induced liver disease.
- Radiation Safety: Reassure and educate about radiation exposure risks, emphasizing that Y-90’s beta emission is largely confined to the treatment site, but certain precautions may be necessary.
Physical and Psychological Preparation
- Medical History and Assessment: Obtain a comprehensive health history, including allergies, previous treatments, comorbidities, and risk factors for liver failure.
- Baseline Assessment: Complete a baseline assessment of vital signs, pain level, neurological status, and skin integrity.
- Venous Access: Ensure patency of intravenous access for medication administration and hydration.
- Psychosocial Support: Address anxiety, answer questions, and provide emotional support. Offer resources such as counseling or support groups if appropriate.
Pre-Procedural Checks
- Laboratory Results: Review and document relevant laboratory values. Inform the medical team of any abnormal findings.
- Medications: Confirm adherence to medication instructions. Administer pre-procedure medications as ordered (e.g., antiemetics, pain medication).
- Consent: Ensure signed informed consent is present in the patient’s records.
- Allergies and Sensitivities: Confirm any allergies, especially to contrast agents used during mapping angiography.
Intra-Procedural Nursing Care
Support and Monitoring
- Patient Reassurance: Provide calm and reassuring presence during the procedure. Clarify steps as they occur, if permitted.
- Vital Sign Monitoring: Continuously monitor vital signs, oxygen saturation, and cardiac rhythm. Report any deviations to the interventional radiology team.
- Observation for Complications: Watch for signs of allergic reaction, pain, or hemodynamic instability.
- Radiation Safety Protocols: Follow institutional protocols for radiation safety, including use of personal protective equipment and limiting exposure time.
Collaboration and Documentation
- Record Keeping: Accurately document the procedure, times, medications administered, patient reactions, and any complications.
- Teamwork: Collaborate closely with interventional radiologists, nuclear medicine specialists, and other health care professionals.
Post-Procedure Nursing Care
Immediate Post-Procedural Monitoring
- Observation: Transfer the patient to a monitored setting. Assess for bleeding at the catheter insertion site, hematoma, or infection.
- Vital Signs: Monitor vital signs at regular intervals as per protocol, including neurological and pain assessments.
- Pain and Nausea Management: Administer prescribed analgesics and antiemetics as needed.
- Hydration: Maintain adequate hydration to aid in the elimination of contrast material and to support renal function.
- Radiation Precautions: Depending on institutional policy, enforce limited patient contact for a short period and provide guidance on waste disposal (e.g., urine, feces containing minimal Y-90 material).
Patient Education and Discharge Planning
- Side Effects: Educate the patient to expect some fatigue, mild fever, and abdominal discomfort, which are typically self-limiting.
- Signs of Complications: Instruct on symptoms that require immediate medical attention, such as severe abdominal pain, jaundice, vomiting blood, or unexplained fever.
- Activity and Diet: Advise on gradual return to activity as tolerated. No special dietary restrictions are usually needed, but a balanced diet is encouraged.
- Follow-Up: Stress the importance of follow-up appointments for imaging, laboratory evaluation, and assessment of treatment response.
Long-Term Monitoring and Support
Assessment of Treatment Response
- Clinical Monitoring: Regular follow-up visits to assess for tumor response, liver function, and overall health.
- Radiologic Evaluation: Imaging studies such as CT, MRI, or PET scans are scheduled to evaluate the effectiveness of therapy and identify any new lesions.
- Laboratory Tests: Monitor liver enzymes, bilirubin, and renal function to detect early signs of toxicity or liver dysfunction.
Management of Late Effects and Complications
- Radiation-Induced Liver Disease: Watch for signs of new or worsening liver failure, ascites, coagulopathy, or encephalopathy. Immediate referral to the medical team is warranted if suspected.
- Biliary Complications: Be vigilant for biliary obstruction or cholangitis.
- Lung Shunting: Rarely, microspheres may shunt to the lungs, causing radiation pneumonitis. Monitor for shortness of breath and respiratory symptoms.
- Psychosocial Support: Continue to provide or refer for counseling, especially for patients with poor prognosis or those experiencing anxiety, depression, or social isolation.
Radiation Safety for Staff and Family
Staff Precautions
- Follow institutional safety protocols for handling radioactive materials.
- Use personal protective equipment as recommended.
- Minimize time spent near radioactive patients when feasible, and maximize distance.
- Participate in mandatory radiation safety training.
Family and Visitor Safety
- Inform family members about any temporary restrictions on close contact, especially with children or pregnant individuals.
- Provide written instructions on hygiene practices and waste disposal, if necessary.
- Reassure that the risk of radiation exposure to others is minimal but not zero, especially shortly after treatment.
Ethical and Legal Considerations
- Ensure informed consent is truly informed, including discussion of alternatives and risks.
- Respect patient autonomy and cultural needs.
- Maintain confidentiality and privacy, especially regarding cancer diagnosis and treatment.
REFERENCES
- Laidlaw GL, Johnson GE. Recognizing and Managing Adverse Events in Y-90 Radioembolization. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8497076/. Semin Intervent Radiol. 2021 Oct;38(4):453-459.
- Sharma NK, Kappadath SC, Chuong M, et al. The American Brachytherapy Society consensus statement for permanent implant brachytherapy using Yttrium-90 microsphere radioembolization for liver tumors. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10868645/. Brachytherapy. 2022Sep-Oct;21(5):569-591.
- Vanani NB, Janardan A, Asmi N, Jha P. Post-embolization Syndrome Following Yttrium-90 Radiation Segmentectomy. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10082639/#:~:text=Post%2Dembolization%20syndrome%20(PES),72%20hours%20after%20the%20procedure.). Cureus. 2023 Mar;15(3):e35947
- Villalobos A, Pisanie JLD, Gandhi RT, Kokabi N. Yttrium-90 Radioembolization Dosimetry: Dose Considerations, Optimization, and Tips. Semin Intervent Radiol. 2024 Mar 14;41(1):63-78. doi: 10.1055/s-0044-1779715. PMID: 38495257; PMCID: PMC10940044.
- Williams SJ, Rilling WS, White SB. Quality of Life and Cost Considerations: Y-90 Radioembolization. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8497083/. Semin Intervent Radiol. 2021 Oct;38(4):482-487.
- Lee HM, Alder L, Nguyen M, Dougherty SC, Qu Y, Thacker LR, Poklepovic A. Long-term outcome analysis of Y90 radioembolization in hepatocellular carcinoma. J Gastrointest Oncol. 2023 Jun 30;14(3):1378-1391. doi: 10.21037/jgo-22-882. Epub 2023 May 11. PMID: 37435218; PMCID: PMC10331743.
- Yu CY, Huang PH, Tsang LL, et al. Yttrium-90 Radioembolization as the Major Treatment of Hepatocellular Carcinoma. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9843618/#:~:text=The%20disease%20control%20rate%20was,year%20overall%20survival%20being%20100%25.. J Hepatocell Carcinoma. 2023 Jan;10:17-26.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


