


Last Updated on January 11, 2026 by Nurseslab.in Editorial Team
Chronic bronchitis is a long‑term inflammatory airway condition marked by persistent productive cough for at least three months over two consecutive years. Understanding its causes, symptoms, diagnosis, and management is essential in nursing, respiratory care, and clinical practice.
Introduction
Chronic bronchitis is a significant respiratory condition that affects millions worldwide, contributing to substantial morbidity and impacting the quality of life of individuals and their families. The most common symptom is a frequent cough that lasts for two years or longer. Chronic bronchitis never really goes away but can be managed with treatment. It’s almost always caused by smoking.
Definition and Overview
What is Chronic Bronchitis?
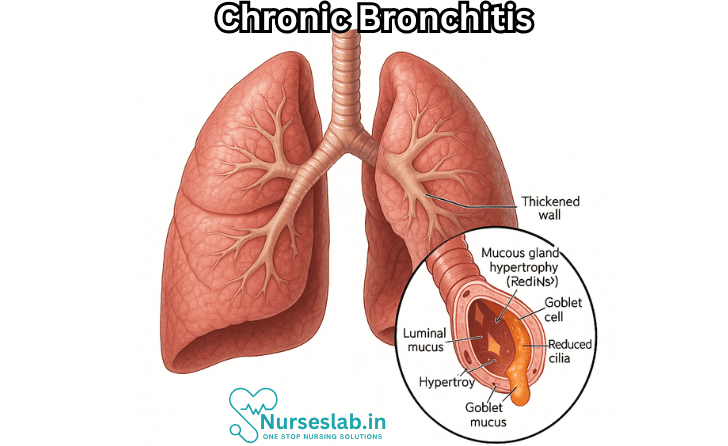
Chronic bronchitis is a persistent inflammation of the bronchi—the large air passages in the lungs—characterised by a productive cough that lasts for at least three months in two consecutive years, in the absence of other causes of chronic cough. It is classified under chronic obstructive pulmonary disease (COPD), a group of progressive lung disorders that impede airflow and breathing.
Acute vs. Chronic Bronchitis
While both acute and chronic bronchitis involve inflammation of the bronchial tubes, they differ fundamentally in duration and underlying cause. Acute bronchitis is typically short-lived, often resulting from viral infections, and resolves within weeks. In contrast, chronic bronchitis is a long-term condition, frequently associated with exposure to irritants such as tobacco smoke and environmental pollutants. The persistent nature of chronic bronchitis leads to ongoing airway inflammation and structural changes in the lungs.
Epidemiology
Chronic bronchitis is prevalent globally, with higher incidence in smokers and individuals exposed to environmental irritants. In India, as well as worldwide, the burden of chronic bronchitis continues to rise, especially in urban areas with increased air pollution. The condition is more common in adults over 40 years of age, and men tend to be affected more frequently than women, although the gender gap is narrowing due to changes in smoking patterns.
Causes and Risk Factors
Smoking
Cigarette smoking remains the leading cause of chronic bronchitis. The inhaled chemicals in tobacco smoke irritate the bronchial lining, triggering inflammatory responses and excessive mucus production. Both active and passive smoking (second-hand smoke exposure) elevate the risk of developing chronic bronchitis.
Environmental Factors
Prolonged exposure to airborne pollutants—such as industrial emissions, vehicle exhaust, and indoor air contaminants like biomass fuel smoke—contributes significantly to the development of chronic bronchitis. In India, the use of wood, coal, and dung for cooking in poorly ventilated homes is a notable risk factor, especially among women.
Genetics
Genetic predisposition plays a role in susceptibility to chronic bronchitis. Individuals with a family history of respiratory diseases may be more prone to developing chronic bronchitis, although environmental factors often interact with genetic risk.
Occupational Hazards
Certain occupations carry increased risk due to exposure to dust, fumes, and chemicals. Workers in mining, construction, agriculture, and manufacturing industries are particularly vulnerable. Chronic exposure to these irritants can damage the respiratory tract and lead to chronic bronchitis.
Other Risk Factors
Additional risk factors include a history of frequent respiratory infections during childhood, low socio-economic status, poor nutrition, and compromised immunity. Age is also a significant factor, with older adults at greater risk due to cumulative exposure and declining lung function.
Signs and Symptoms
Chronic Cough
A hallmark of chronic bronchitis is a persistent, productive cough, often described as “smoker’s cough.” The cough is typically worse in the mornings and may be accompanied by copious amounts of sputum.
Sputum Production
Individuals with chronic bronchitis frequently expectorate thick, mucoid, or purulent sputum. The colour and consistency of sputum may vary, especially during exacerbations or concurrent infections.
Shortness of Breath
Progressive breathlessness, particularly on exertion, is common. In advanced cases, patients may experience dyspnoea even at rest, significantly limiting physical activity.
Other Symptoms
Additional symptoms may include wheezing, chest discomfort, fatigue, and recurrent respiratory infections. The severity of symptoms often fluctuates, with periods of relative stability interspersed with acute exacerbations.
Progression of Symptoms
Over time, chronic bronchitis can lead to worsening airway obstruction, increased frequency of exacerbations, and diminished exercise tolerance. The progressive nature of the disease underscores the importance of early recognition and intervention.
Diagnosis
Medical History
Diagnosis begins with a thorough medical history, focusing on the duration and characteristics of cough, exposure to risk factors, and previous respiratory illnesses. Enquiry into smoking habits, occupational exposures, and family history is essential.
Physical Examination
Clinical examination may reveal wheezing, crackles (rales), and prolonged expiratory phase. Signs of respiratory distress, cyanosis, or clubbing indicate advanced disease.
Pulmonary Function Tests
Spirometry is the gold standard for assessing lung function in chronic bronchitis. It measures forced expiratory volume in one second (FEV1) and forced vital capacity (FVC), helping to quantify the degree of airflow obstruction and monitor disease progression.
Imaging Studies
Chest X-rays can help exclude other causes of chronic cough and detect complications such as pneumonia or lung hyperinflation. High-resolution computed tomography (CT) scans may be employed for detailed assessment in complex cases.
Laboratory Tests
Sputum analysis may be performed to identify infectious agents during exacerbations. Blood tests, including complete blood count and arterial blood gases, can assess the extent of hypoxaemia and rule out comorbid conditions.
Diagnostic Criteria
The diagnosis of chronic bronchitis is clinical, based on history and physical findings. However, ancillary tests are crucial for excluding other diseases and guiding management.
Treatment Options
Medications
Pharmacological therapy aims to relieve symptoms, reduce exacerbations, and improve lung function. Commonly used medications include:
- Bronchodilators: Beta-agonists and anticholinergic agents relax airway muscles, easing breathing.
- Corticosteroids: Inhaled corticosteroids reduce airway inflammation, but their long-term use requires careful monitoring due to potential side effects.
- Mucolytics: These agents help thin and clear mucus, facilitating expectoration.
- Antibiotics: Indicated during acute exacerbations associated with bacterial infections.
Pulmonary Rehabilitation
Structured pulmonary rehabilitation programmes combine exercise training, education, and psychosocial support. These programmes improve exercise tolerance, reduce symptoms, and enhance quality of life.
Lifestyle Modifications
Lifestyle changes are central to managing chronic bronchitis. Smoking cessation is paramount and may require behavioural interventions, counselling, and pharmacotherapy. Nutritional support and regular physical activity contribute to overall well-being.
Oxygen Therapy
Patients with advanced disease and persistent hypoxaemia may benefit from supplemental oxygen therapy. Long-term oxygen use can prevent complications such as pulmonary hypertension and improve survival.
Surgical Options
Surgical interventions, such as lung volume reduction surgery or lung transplantation, are reserved for selected patients with severe, refractory disease who do not respond to medical management.
Management of Exacerbations
Prompt recognition and treatment of acute exacerbations are vital to prevent hospitalisation and further lung damage. This may involve short courses of antibiotics, corticosteroids, and increased bronchodilator use.
Prevention Strategies
Smoking Cessation
Quitting smoking is the most effective way to prevent chronic bronchitis and slow its progression. Public health campaigns, support groups, and smoking cessation clinics play a crucial role in helping individuals overcome nicotine addiction.
Reducing Exposure to Irritants
Minimising exposure to indoor and outdoor air pollutants is essential. Using cleaner cooking fuels, improving ventilation, and wearing protective equipment in hazardous workplaces can reduce risk.
Vaccinations
Immunisation against influenza and pneumococcal infections is recommended for individuals with chronic bronchitis, as these infections can precipitate exacerbations and worsen outcomes.
Healthy Lifestyle Choices
Adopting a balanced diet, engaging in regular exercise, and maintaining optimal body weight support lung health and reduce susceptibility to infections.
Early Detection and Intervention
Regular health check-ups and prompt attention to respiratory symptoms enable early diagnosis and intervention, potentially preventing disease progression.
Complications
Respiratory Failure
Chronic bronchitis can lead to progressive lung impairment and respiratory failure, characterised by inadequate oxygenation and carbon dioxide retention. This is a life-threatening complication requiring intensive medical intervention.
Pulmonary Hypertension
Persistent low oxygen levels may cause increased pressure in the pulmonary arteries, leading to pulmonary hypertension. This condition strains the right side of the heart and can result in heart failure.
Frequent Infections
Damaged airways and impaired mucociliary clearance increase susceptibility to recurrent respiratory infections, which can further accelerate lung damage.
Impact on Comorbidities
Chronic bronchitis often coexists with other medical conditions, such as cardiovascular disease, diabetes, and osteoporosis. The interplay between these diseases can complicate management and worsen outcomes.
Other Complications
Additional complications include acute exacerbations, pneumonia, and decreased exercise capacity. These issues contribute to increased healthcare utilisation and diminished quality of life.
Impact on Quality of Life
Physical Aspects
Chronic bronchitis imposes significant physical limitations. Breathlessness, fatigue, and reduced exercise tolerance hinder daily activities, leading to dependency and loss of independence.
Emotional and Psychological Impact
Living with a chronic respiratory disease can be distressing. Patients may experience anxiety, depression, and feelings of isolation. The unpredictable nature of exacerbations and progressive decline can affect mental health.
Social Implications
The disease often disrupts social interactions, employment, and family dynamics. Frequent hospitalisations and absenteeism from work or school can result in financial strain and reduced social participation.
Coping Strategies
Effective coping mechanisms include joining support groups, engaging in pulmonary rehabilitation, and seeking professional counselling. Education and self-management empower patients to take control of their condition and improve their quality of life.
Nursing Care of a Patient with Chronic Bronchitis
Effective nursing care for patients with chronic bronchitis is crucial in relieving symptoms, slowing disease progression, preventing complications, and improving quality of life.
Assessment of the Patient
Nursing care begins with a thorough assessment, which involves:
- Health history: Documenting smoking history, occupational exposure, frequency and duration of symptoms, previous hospitalizations, and current medications.
- Physical examination: Observing for signs such as cyanosis, use of accessory muscles, increased anteroposterior chest diameter (“barrel chest”), and auscultating lung sounds for wheezing, crackles, or rhonchi.
- Psychosocial assessment: Assessing anxiety, depression, social support systems, and coping mechanisms.
- Laboratory and diagnostic tests: Monitoring arterial blood gases (ABG), pulmonary function tests (PFTs), chest X-ray, and sputum culture if infection is suspected.
Nursing Diagnoses for Chronic Bronchitis
Common nursing diagnoses in chronic bronchitis include:
- Ineffective airway clearance related to excessive mucus production.
- Impaired gas exchange related to airway obstruction and alveolar hypoventilation.
- Activity intolerance related to imbalance between oxygen supply and demand.
- Risk for infection related to impaired pulmonary defense mechanisms.
- Ineffective breathing pattern related to inflammation and bronchoconstriction.
- Deficient knowledge related to disease process, management, and prevention.
Planning and Outcome Identification
The primary goals of nursing care are:
- Maintain a patent airway and optimize gas exchange.
- Reduce frequency and severity of exacerbations.
- Promote independence in activities of daily living (ADLs).
- Prevent and manage complications, such as respiratory infections.
- Enhance patient knowledge about disease management and lifestyle modifications.
Nursing Interventions
1. Airway Clearance and Respiratory Function
- Encourage effective coughing techniques: Teach huff coughing and controlled coughing to mobilize secretions.
- Hydration: Encourage oral fluids (unless contraindicated) to thin secretions, making them easier to expectorate.
- Chest Physiotherapy: Perform percussion, vibration, and postural drainage as indicated to facilitate mucus movement.
- Administer bronchodilators and mucolytics: As prescribed, to reduce bronchospasm and loosen mucus.
- Monitor respiratory rate, depth, and pattern: Report changes promptly to detect early deterioration.
- Provide supplemental oxygen: As ordered, ensuring cautious administration (usually low-flow) to avoid suppressing hypoxic drive in CO2 retainers.
- Suctioning: When necessary, use sterile technique to clear airway, preventing aspiration and infection.
2. Infection Prevention
- Hand hygiene: Emphasize to patient and visitors the critical role of frequent handwashing in reducing infection risk.
- Vaccinations: Encourage annual influenza and pneumococcal vaccinations.
- Monitor for signs of infection: Including fever, increased sputum production or purulence, and worsening dyspnea. Report promptly.
- Promote oral care: Reduce colonization of pathogens that can be aspirated into the lungs.
3. Patient Education and Health Promotion
- Smoking cessation support: Provide resources, counseling, and, if needed, pharmacological aids to encourage quitting.
- Medication adherence: Instruct on proper inhaler and nebulizer techniques. Emphasize the importance of taking medications as prescribed, even in the absence of symptoms.
- Recognizing exacerbations: Teach the patient how to identify early signs and symptoms of worsening condition and when to seek medical advice.
- Energy conservation techniques: Advise on balancing activity with rest, pacing, and prioritizing tasks to minimize fatigue.
- Nutritional support: Encourage small, frequent, high-calorie meals if weight loss is an issue. Collaborate with a dietitian as necessary.
- Environmental control: Advise on reducing exposure to respiratory irritants such as smoke, dust, strong odors, and temperature extremes.
4. Psychological Support
- Anxiety reduction: Use relaxation techniques, breathing exercises, and reassurance to help manage anxiety and breathlessness.
- Provide social support: Connect patients to support groups and community resources for those living with chronic lung disease.
- Address depression or isolation: Screen for mood changes and refer for counseling or therapy if needed.
5. Promoting Activity and Independence
- Assess tolerance to activity: Use tools such as the Borg scale and monitor oxygen saturation during and after activity.
- Encourage participation in pulmonary rehabilitation programs: These programs improve exercise capacity and quality of life.
- Assist with ADLs as needed, but foster independence: Allow the patient to do for themselves what they are able to, providing rest periods between activities.
Evaluation of Care
Evaluation involves assessing the effectiveness of interventions and progress toward established goals. This may include:
- Improved breath sounds, less coughing and sputum production.
- Stable or improved oxygen saturation levels.
- Reduced frequency of exacerbations and hospitalizations.
- Increased participation in ADLs and improved exercise tolerance.
- Enhanced patient understanding of disease management and lifestyle changes.
Special Considerations
- Older adults: May have additional comorbidities and reduced physiological reserves. Tailor interventions accordingly.
- Polypharmacy: Monitor for potential drug interactions and side effects.
- Home care planning: Arrange for follow-up, home oxygen if required, and ensure the patient and caregivers are competent in disease self-management.
- Palliative care: For advanced disease, focus may shift to symptom relief and quality of life.
REFERENCES
- Ambrosino N, et al. Lifestyle interventions in prevention and comprehensive management of COPD. Breathe. 2018; doi:10.1183/20734735.018618.
- American Lung Association. Chronic Bronchitis. https://www.lung.org/lung-health-diseases/lung-disease-lookup/chronic-bronchitis.
- Bennett NL. Chronic Obstructive Pulmonary Disease (COPD). In: Stern SC, Cifu AS, Altkorn D, eds. Symptom to Diagnosis: An Evidence-Based Guide, 4e. McGraw Hill; 2020.
- Ferri FF. Acute bronchitis. In: Ferri’s Clinical Advisor 2021. Elsevier; 2021. https://www.clinicalkey.com.
- Kim V, Criner GJ. Chronic bronchitis and chronic obstructive pulmonary disease.. https://pubmed.ncbi.nlm.nih.gov/23204254/Am J Respir Crit Care Med. 2013 Feb 1;187(3):228-37.
- Sisson TH, Claar D, Chesnutt MS, Prendergast TJ. Pulmonary Disease. In: Hammer GD, McPhee SJ, eds. Pathophysiology of Disease: An Introduction to Clinical Medicine, 8e. McGraw Hill; 2019.
- CDC, How to prevent the spread of respiratory illnesses in disaster evacuation centers. Centers for Disease Control and Prevention. https://www.cdc.gov/disasters/disease/respiratoryic.html
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


