


Last Updated on January 22, 2026 by Nurseslab.in Editorial Team
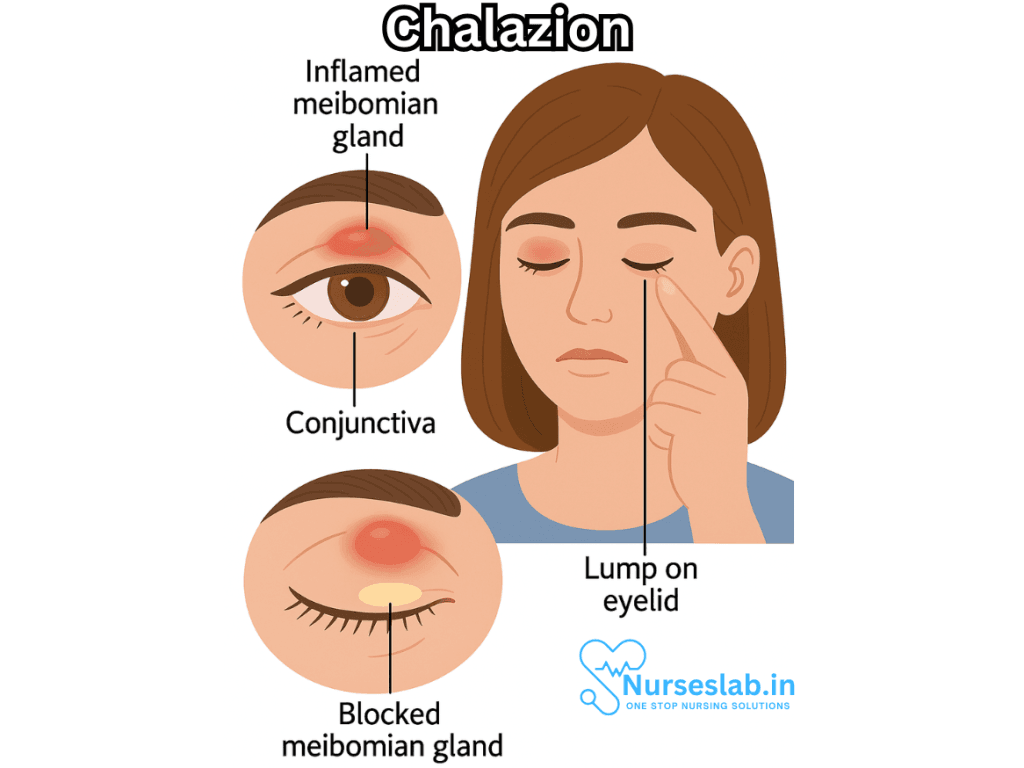
A chalazion is a common, non-infectious, benign lump or swelling that occurs on the eyelid due to the blockage and inflammation of a meibomian gland. These oil-secreting glands are located within the tarsal plate of the eyelids and play a crucial role in maintaining a healthy tear film and lubricating the eye’s surface. While often mistaken for a stye (hordeolum), a chalazion differs in several key aspects, including its underlying cause and clinical course.
What is a Chalazion?
A chalazion (plural: chalazia) appears as a localized swelling or lump, typically on the upper or lower eyelid. It results from the obstruction of a meibomian gland duct, leading to the retention of sebaceous secretions and subsequent chronic inflammation. Unlike a stye, which is usually painful and caused by an acute bacterial infection of the eyelid glands, a chalazion develops more slowly, is usually painless, and is not primarily due to infection.
Causes and Pathophysiology
The eyelids contain dozens of meibomian glands that secrete an oily substance called meibum. This substance is essential for preventing the evaporation of the eye’s tear film and maintaining ocular comfort. When the duct of a meibomian gland becomes blocked, meibum accumulates and triggers a granulomatous inflammatory response. This response is characterized by the infiltration of immune cells, particularly macrophages and giant cells, forming a palpable nodule.
Common causes and contributing factors include:
- Meibomian gland dysfunction: Chronic alteration in gland function can predispose to blockage.
- Blepharitis: Chronic inflammation of the eyelid margin can increase the risk for chalazion formation.
- Skin conditions: Rosacea, seborrheic dermatitis, and acne vulgaris are associated with increased risk due to changes in glandular secretions.
- Poor eyelid hygiene: Accumulation of debris and oil can increase the likelihood of gland obstruction.
- Previous history: Individuals with a history of chalazia are at higher risk for recurrence.
Symptoms and Clinical Presentation
A chalazion typically develops gradually over several days to weeks. The hallmark features include:
- Painless, localized swelling or lump on the eyelid (upper more commonly than lower)
- Firm, round nodule within the tarsal plate of the eyelid
- Mild tenderness may be present during initial development but usually subsides
- Redness and swelling of the overlying skin or conjunctiva
- Blurred vision if the nodule is large enough to press against the cornea
- Rarely, secondary infection can occur, leading to increased pain and redness
While most chalazia are asymptomatic, larger lesions may cause cosmetic concerns or mechanical ptosis (drooping of the eyelid). In rare cases, patients may experience recurrent or multiple chalazia, which warrants evaluation for underlying conditions.
Chalazion vs. Stye (Hordeolum): Key Differences
It is important to distinguish between a chalazion and a stye, as their treatment and prognosis differ:
- Chalazion: Chronic, non-infectious, usually painless, arises from meibomian gland obstruction, forms away from the eyelid margin.
- Stye (Hordeolum): Acute, infectious (commonly Staphylococcus aureus), painful, involves lash follicles or glands of Zeis/Moll, occurs at the eyelid margin.
Diagnosis
Diagnosis is generally clinical, based on history and examination of the eyelid. The features a clinician looks for include:
- Palpable, firm, non-tender nodule within the tarsal plate
- Absence of acute pain or purulent discharge (unless secondarily infected)
- No systemic symptoms
In atypical cases or cases refractory to treatment, further evaluation may be warranted to rule out malignancy (e.g., sebaceous gland carcinoma), especially in older adults or those with recurrent lesions in the same location.
Treatment and Management
Most chalazia resolve spontaneously within a few weeks with conservative management. The mainstay of initial treatment includes:
- Warm compresses: Applying a clean, warm compress to the affected eyelid for 10-15 minutes, 3-6 times daily, helps soften the contents and promotes drainage.
- Gentle eyelid massage: Massaging the eyelid after warm compresses can help unblock the gland.
- Eyelid hygiene: Regular cleaning of the eyelid margins with diluted baby shampoo or commercial eyelid cleansers reduces the risk of recurrence.
- Avoid squeezing or attempting to “pop” the lesion: This can cause trauma or secondary infection.
If the chalazion persists beyond 4 weeks or causes significant discomfort, further interventions may be considered:
- Topical corticosteroids: These may be prescribed to reduce inflammation (under medical supervision).
- Intralesional steroid injection: Injection of corticosteroids directly into the chalazion may hasten resolution, especially for small- to medium-sized lesions.
- Surgical incision and curettage: For large, persistent, or cosmetically concerning chalazia, minor surgery under local anesthesia is effective and safe.
- Antibiotics: Only indicated if secondary infection is suspected.
Complications
Although most chalazia are benign, some complications can occur:
- Secondary infection resulting in abscess formation
- Cosmetic deformity
- Ptosis (drooping of the eyelid)
- Astigmatism or blurred vision due to corneal pressure from a large lesion
- Rarely, persistent or recurrent chalazia may be misdiagnosed or mask underlying malignancy
Prevention
Preventive measures focus on maintaining eyelid hygiene and addressing underlying risk factors:
- Regular cleansing of eyelid margins, especially for those prone to blepharitis or with a history of chalazion
- Managing seborrheic dermatitis, rosacea, and other skin conditions
- Avoiding eye makeup or products that may clog the glands if sensitive
- Promptly treating styes or eyelid inflammation to prevent progression
When to See a Healthcare Provider
Most chalazia are harmless and resolve on their own, but medical attention is advised if:
- The lesion persists for more than a month
- There is significant pain, redness, or swelling suggestive of infection
- Vision becomes affected
- There are recurrent or multiple lesions
- There is any concern for malignancy (especially in older adults or atypical cases)
Prognosis
The prognosis for most chalazia is excellent. With conservative management, most resolve within a few weeks to months. Surgical removal is curative in nearly all persistent cases. Recurrence is possible, especially in individuals with underlying skin or eyelid conditions, highlighting the importance of ongoing eyelid hygiene.
Nursing Care of a Patient with Chalazion
As frontline caregivers, nurses hold a pivotal role in both the management and education of patients suffering from chalazion, ensuring effective treatment, comfort, and prevention of complications.
Nursing Assessment
Nursing care begins with a thorough assessment, which should include:
- Health History: Ask about the onset, duration, and progression of the eyelid swelling, presence of pain, previous episodes, and risk factors such as blepharitis, rosacea, or chronic eye conditions.
- Physical Examination: Observe for swelling, redness, and note the size, location, and consistency of the eyelid lesion. Assess both upper and lower lids. Check for signs of infection or cellulitis, such as warmth, tenderness, and purulent discharge.
- Visual Acuity: Evaluate if the lesion is large enough to impact the patient’s vision. Screen for visual blurring or astigmatism.
- Psychosocial Impact: Assess how the lesion affects the patient’s self-esteem, social interactions, and daily activities, particularly in children and adolescents.
Nursing Diagnosis
Common nursing diagnoses for a patient with chalazion may include:
- Acute discomfort or pain related to eyelid inflammation
- Disturbed body image related to visible swelling on eyelid
- Risk of infection related to manipulation or improper hygiene
- Knowledge deficit regarding home care and prevention
Nursing Interventions
Effective nursing care for chalazion focuses on symptom relief, preventing complications, educating the patient, and supporting recovery. The following interventions are essential:
1. Symptom Relief and Conservative Management
- Warm Compresses: Instruct the patient to apply a clean, warm compress (such as a cloth soaked in warm water) to the affected eyelid for 10–15 minutes, 3–5 times daily. This helps soften the blocked secretions and promotes spontaneous drainage.
- Lid Hygiene: Teach gentle cleansing of the eyelid with diluted baby shampoo or prescribed eyelid scrubs to reduce debris and prevent further blockage or infection.
- Avoid Squeezing: Advise the patient not to squeeze, rub, or attempt to ‘pop’ the lump, as this may aggravate inflammation or introduce infection.
- Analgesia: If mild discomfort is present, recommend using over-the-counter pain relievers such as acetaminophen or ibuprofen, as prescribed and appropriate.
2. Infection Surveillance
- Monitor for signs of secondary infection, including increasing redness, swelling, tenderness, warmth, or discharge. Promptly report any suspicion of infection to the healthcare provider, as this may warrant antibiotic therapy or further intervention.
- Document any systemic symptoms (fever, malaise) that may indicate spread of infection, such as preseptal cellulitis.
3. Patient Education
Patient education is a cornerstone of nursing care for chalazion. Key teaching points include:
- Proper Application of Warm Compresses: Demonstrate the correct way to apply compresses and stress the importance of regularity for optimal results.
- Eyelid Hygiene: Educate about daily eyelid cleansing, especially in patients with risk factors like blepharitis or acne rosacea. Stress the avoidance of sharing towels and pillows to minimize contamination.
- When to Seek Medical Attention: Advise the patient to return if the lesion enlarges, persists beyond two weeks, becomes increasingly painful, or is associated with vision changes or systemic symptoms.
- Medication Adherence: If topical antibiotics or steroid ointments are prescribed, explain the correct dosage, application method, and duration of therapy. Warn about possible side effects.
- Prevention of Recurrence: Discuss the importance of lid hygiene in preventing future episodes, especially for those with chronic conditions.
4. Emotional and Psychological Support
- Be attentive to the patient’s feelings about cosmetic appearance, especially in adolescents and those in public-facing roles. Offer reassurance and, if needed, access to counseling or support groups.
- Encourage open communication about concerns or anxieties related to the condition or its management.
5. Pre- and Post-Procedure Care
If conservative management fails and surgical intervention is required (such as incision and curettage), the nurse’s responsibilities include:
Pre-Procedure:
- Prepare the patient for the minor procedure, explaining the steps, anesthesia, and expected outcomes.
- Ensure informed consent is obtained and all pre-procedure protocols are followed.
- Assess for allergies to local anesthesia or antiseptics.
Post-Procedure:
- Monitor for complications such as bleeding, infection, or recurrence.
- Teach wound care: keeping the area clean, applying prescribed ointments, and avoiding eye makeup or contact lenses until healing occurs.
- Arrange for follow-up appointments and address any concerns regarding recovery and prevention.
Special Considerations
- Pediatric Patients: Children may have difficulty adhering to compress routines or avoiding eye rubbing. Family education and support are essential.
- Patients with Recurrent Chalazia: Assess for underlying conditions such as meibomian gland dysfunction, seborrheic dermatitis, or systemic diseases that may require specialist referral.
- Immunocompromised Patients: These individuals may be at higher risk for infection or complications; vigilant monitoring and early intervention are warranted.
Documentation
Accurate and comprehensive documentation supports continuity of care and legal protection. Key points to document include:
- Description of the chalazion: size, location, duration, associated symptoms
- Patient’s reported levels of discomfort or pain
- Education provided and patient’s understanding of instructions
- Response to nursing interventions
- Referral to ophthalmology or other health professionals if indicated
Multidisciplinary Collaboration
Collaboration with ophthalmologists, primary care providers, and pharmacists ensures holistic care. Timely referral is needed if the chalazion does not resolve, recurs frequently, or if malignancy is suspected (rare in older adults). Nurses should also liaise with family members or caregivers as appropriate to support home care adherence.
Prevention Tips
- Encourage regular eyelid hygiene for at-risk individuals
- Prompt treatment of blepharitis or skin conditions affecting eyelid margins
- Avoid sharing personal items like towels and eye cosmetics
- Routine eye check-ups for individuals with recurrent or chronic eyelid issues
REFERENCES
- American Academy of Dermatology. How to Treat Boils and Styes. https://www.aad.org/public/everyday-care/injured-skin/treat-boils-styes.
- Zhu Y, Zhao H, Huang X, et al. Novel treatment of chalazion using light-guided-tip intense pulsed light. Sci Rep. 2023;13(1):12393. doi:10.1038/s41598-023-39332-x
- American Academy of Ophthalmology. What Is the Difference Between a Stye and a Chalazion? Causes, Symptoms, Treatment. https://www.aao.org/eye-health/diseases/what-are-chalazia-styes. Last reviewed 6/14/2023.
- American Association for Pediatric Ophthalmology and Strabismus. Chalazion. https://aapos.org/glossary/chalazion. Last updated 11/2021.
- American Optometric Association. Chalazia. https://www.aoa.org/healthy-eyes/eye-and-vision-conditions/chalazion?sso=y.
- Alsuhaibani AH, Al-Faky YH. Large anterior orbital cyst as a late complication of chalazion surgical drainage. Eye (Lond). 2015;29(4): 585–587. doi:10.1038/eye.2014.339
- Jordan GA, Beier K. Chalazion. https://www.ncbi.nlm.nih.gov/books/NBK499889/. [Updated 2023 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-.
- Merck Manual (Consumer Version). Chalazion and Stye (Hordeolum). https://www.merckmanuals.com/home/eye-disorders/eyelid-and-tearing-disorders/chalazion-and-stye-hordeolum. Last modified 9/2022.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


