


Introduction
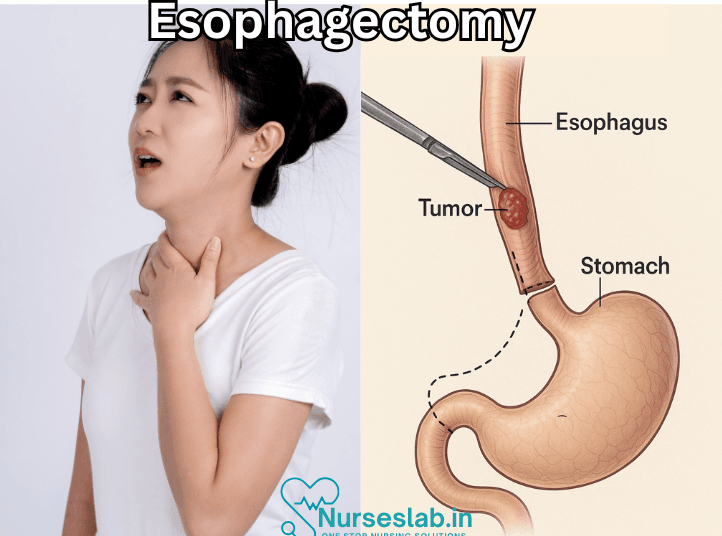
Esophagectomy is a surgical procedure that involves the removal of part or all of the esophagus, the muscular tube that connects the throat to the stomach. Esophagectomy Surgery is most commonly performed to treat esophageal cancer but can also be used for other conditions such as severe gastroesophageal reflux disease (GERD), Barrett’s esophagus, esophageal strictures, and achalasia.
Types of Esophagectomy
There are several types of esophagectomy, each with specific indications and techniques:
Transhiatal Esophagectomy
This approach involves removing the esophagus through incisions in the neck and abdomen. It avoids the need for a chest incision, which can reduce recovery time and postoperative complications.
Transthoracic Esophagectomy
In this procedure, the surgeon makes an incision in the chest to access the esophagus. It allows for a more direct view and access to the esophagus but may involve longer recovery times and higher risks.
Minimally Invasive Esophagectomy
This technique uses small incisions and specialized instruments to perform the surgery, resulting in less trauma to the body, reduced pain, and faster recovery compared to traditional open surgery.
Indications for Esophagectomy
Esophagectomy is primarily indicated for the following conditions:
- Esophageal Cancer: It is the most common reason for esophagectomy, especially when the cancer is localized and has not spread to distant organs.
- Barrett’s Esophagus: A precancerous condition where the lining of the esophagus changes due to chronic acid exposure from GERD.
- Severe GERD: When gastroesophageal reflux disease causes significant damage and scarring to the esophagus, making it difficult to manage with medication or other treatments.
- Achalasia: A rare disorder where the esophagus loses its ability to move food toward the stomach, causing severe swallowing difficulties.
- Esophageal Strictures: Narrowing of the esophagus due to scarring from chronic inflammation or injury.
Preoperative Preparation
Before undergoing an esophagectomy, patients should go through a thorough evaluation and preparation process, which includes:
- Medical Assessment: Comprehensive evaluation by a multidisciplinary team, including surgeons, oncologists, and anesthesiologists, to determine the patient’s suitability for surgery.
- Imaging Studies: Tests such as endoscopy, CT scans, and PET scans to assess the extent of the disease and plan the surgical approach.
- Preoperative Optimization: Nutritional support, pulmonary rehabilitation, and other interventions to optimize the patient’s health before surgery.
- Informed Consent: Detailed discussion with the patient about the risks, benefits, and expected outcomes of the procedure.
Surgical Procedure
The esophagectomy procedure involves several key steps:
- Anesthesia: The patient is placed under general anesthesia.
- Incisions: Depending on the type of esophagectomy, incisions are made in the neck, chest, and/or abdomen.
- Removal of the Esophagus: The affected portion of the esophagus is carefully removed.
- Reconstruction: The stomach or a section of the intestine is used to create a new passage for food, which is connected to the remaining esophagus or directly to the throat.
- Closure: The incisions are closed, and drainage tubes may be placed to remove excess fluids.
Postoperative Care
Recovery from an esophagectomy requires careful management and monitoring:
- Hospital Stay: Patients typically stay in the hospital for 7-10 days, with close monitoring in an intensive care unit initially.
- Pain Management: Pain relief is provided through medications and, in some cases, epidural analgesia.
- Nutritional Support: Initially, patients may receive nutrition through a feeding tube, transitioning to a liquid diet and then to solid foods as tolerated.
- Respiratory Care: Breathing exercises and physical therapy to prevent complications such as pneumonia.
- Follow-up: Regular follow-up visits to monitor recovery, manage any complications, and assess for recurrence of disease in cancer patients.
Risks and Complications
As with any major surgery, esophagectomy carries certain risks and potential complications, including:
- Anastomotic Leak: Leakage at the site where the new esophageal passage is connected.
- Infection: Risk of infections at the surgical site or in the chest.
- Respiratory Complications: Pneumonia, atelectasis, or respiratory failure.
- Strictures: Narrowing of the newly constructed passage.
- Bleeding: Risk of significant blood loss during or after surgery.
- Gastrointestinal Issues: Issues such as delayed gastric emptying or reflux.
Outcomes and Prognosis
The outcomes and prognosis after an esophagectomy vary depending on the underlying condition, the stage of disease (in the case of cancer), and the patient’s overall health. Advances in surgical techniques and postoperative care have improved the survival rates and quality of life for many patients undergoing this procedure.
Nursing Care of Patient with Esophagectomy
Esophagectomy, the surgical removal of the esophagus, is a major procedure often performed to treat esophageal cancer or other severe esophageal diseases. Due to the complexity and the associated risks, specialized nursing care is crucial in ensuring optimal recovery and patient outcomes.
A. Preoperative Care
Patient Education
Informed Consent: Ensure that the patient understands the procedure, potential risks, and expected outcomes.
Preoperative Instructions: Provide guidance on fasting, medication adjustments, and preparation for surgery.
Nutritional Support
Assessment: Evaluate the patient’s nutritional status and provide necessary supplements.
Dietary Plan: Implement a preoperative diet that optimizes the patient’s health.
B. Postoperative Care
Pain Management
Assessment: Regularly assess pain levels using standardized pain scales.
Medication Administration: Provide appropriate analgesics as prescribed, monitoring for effectiveness and side effects.
Respiratory Support
Respiratory Exercises: Encourage deep breathing and coughing exercises to prevent pneumonia and atelectasis.
Oxygen Therapy: Administer oxygen and monitor saturation levels as needed.
Wound Care
Inspection and Maintenance: Regularly inspect the surgical site for signs of infection or complications and maintain sterile dressings.
Drain Management: Monitor and manage surgical drains to prevent fluid accumulation.
Monitoring for Complications
Anastomotic Leak: Watch for signs of leakage such as fever, chest pain, or subcutaneous emphysema.
Infection: Monitor for signs of infection including redness, swelling, and fever.
Respiratory Complications: Observe for symptoms of pneumonia, atelectasis, or respiratory distress.
Strictures: Be alert for signs of narrowing such as difficulty swallowing or regurgitation.
Bleeding: Monitor for signs of blood loss, including hypotension, tachycardia, and decreased hemoglobin levels.
Gastrointestinal Issues: Watch for delayed gastric emptying or reflux symptoms.
Nutritional Support
Initial Feeding: Begin with clear liquids and gradually progress to soft foods as tolerated.
Tube Feeding: If necessary, provide nutritional support via feeding tubes until oral intake is sufficient.
C. Rehabilitation and Discharge Planning
Physical Therapy
Mobility Exercises: Encourage early ambulation and provide exercises to prevent complications such as deep vein thrombosis.
Patient Education
Discharge Instructions: Provide comprehensive guidelines on medication management, wound care, dietary restrictions, and signs of complications to watch for.
Follow-Up Care: Schedule follow-up appointments to monitor recovery and address any concerns.
REFERENCES
- Bograd AJ, Molena D. Minimally invasive esophagectomy. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9089813/). Curr Probl Surg. 2021 Oct;58(10):100984.
- Townsend CM Jr, et al. Esophagus. In: Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 21st ed. Elsevier; 2022. https://www.clinicalkey.com.
- National Cancer Institute (U.S.). Esophageal Cancer Treatment (PDQ®)-Patient Version. https://www.cancer.gov/types/esophageal/patient/esophageal-treatment-pdq. Updated 11/18/2021.
- Worrell SG, et al. The Society of Thoracic Surgeons/American Society for Radiation Oncology updated clinical practice guidelines on multimodality therapy for locally advanced cancer of the esophagus or gastroesophageal junction. Practical Radiation Oncology. 2024; doi:10.1016/j.prro.2023.10.001.
- Palmieri L, De Giacomo T, Quaresima S, et al. Minimally Invasive Esophagectomy for Esophageal Cancer. (https://www.ncbi.nlm.nih.gov/books/NBK586008/). In: Morgado-Diaz JA, ed. Gastrointestinal Cancers [Internet]. Brisbane (AU): Exon Publications; 2022 Sep 30. Chapter 9.
- Tukanova KH, Chidambaram S, Guidozzi N, Hanna GB, McGregor AH, Markar SR. Physiotherapy Regimens in Esophagectomy and Gastrectomy: a Systematic Review and Meta-Analysis. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8990957/). Ann Surg Oncol. 2022 May;29(5):3148-3167.
- Ahmadinejad M, et al. Risk factors and therapeutic measures for postoperative complications associated with esophagectomy. Annals of Medicine and Surgery. 2020; doi:10.1016/j.amsu.2020.05.011.
- Watkins AA, Kent MS, Wilson JL. Surgical Adjuncts During Esophagectomy. (https://pubmed.ncbi.nlm.nih.gov/32593364/). Thorac Surg Clin. 2020;30(3):315-320.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


