


Surgical Management of Intestinal Malrotation
Introduction
The Ladd procedure is a surgical operation designed to correct malrotation of the intestines, a congenital anomaly where the intestines do not develop in their typical anatomical position. This operation was first described by Dr. William E. Ladd, a pioneering American pediatric surgeon, in the early 20th century, and remains the standard of care for intestinal malrotation to this day. The Ladd procedure is most commonly performed in infants and young children, although it may occasionally be required in older children or adults who present with symptoms.
Background: Intestinal Malrotation
Intestinal malrotation arises during fetal development, typically between the 4th and 12th weeks of gestation, when the midgut fails to rotate 270 degrees counterclockwise around the superior mesenteric artery. This abnormal positioning can lead to a narrow mesenteric base and predispose patients to volvulus, a potentially life-threatening twisting of the bowel that can cut off blood supply and lead to intestinal necrosis.
- Incidence: Approximately 1 in 500 live births are affected by malrotation, though not all will develop symptoms.
- Symptoms: Symptoms may range from intermittent abdominal pain and vomiting to acute, life-threatening intestinal obstruction and shock. Bilious (green) vomiting in a newborn is a classic warning sign.
- Diagnosis: Diagnosis is often made via imaging studies, such as an upper gastrointestinal series, which may reveal a malpositioned duodenojejunal junction or evidence of volvulus.
Indications for the Ladd Procedure
The Ladd procedure is indicated in all patients diagnosed with malrotation due to the risk of volvulus, even if they are asymptomatic. In emergent situations—especially if volvulus is suspected—the operation is performed without delay because of the risk of bowel ischemia.
Description of the Ladd Procedure
The Ladd procedure can be performed through an open (laparotomy) or minimally invasive (laparoscopic) approach, depending on the patient’s age, clinical stability, and the surgeon’s expertise. The procedure comprises several steps, each designed to reduce the risk of volvulus and alleviate any existing obstructions:
1. Reduction of Volvulus (if present)
If the intestine is twisted (volvulus), the first priority is to untwist the bowel in a counterclockwise direction. This step restores blood flow and minimizes the risk of further ischemia or necrosis.
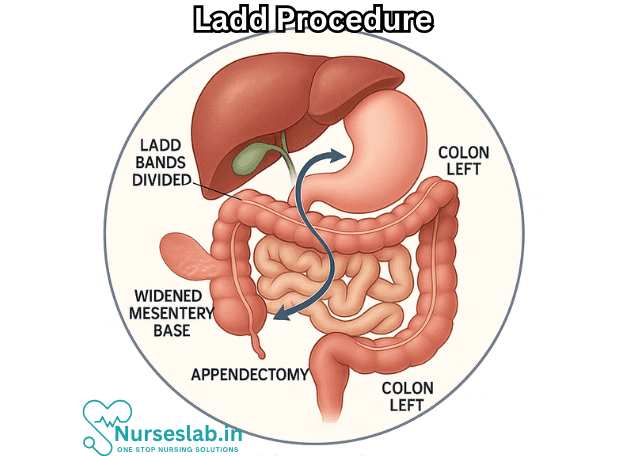
2. Division of Ladd’s Bands
Ladd’s bands are fibrous peritoneal attachments that extend from the malpositioned cecum to the retroperitoneum, often crossing over and compressing the duodenum. These bands are divided to relieve any extrinsic obstruction of the duodenum and to improve the mobility of the intestines.
3. Widening of the Mesenteric Base
Because malrotation results in a narrow mesenteric base, the small and large intestines are repositioned: the small bowel is placed on the right side of the abdomen and the colon on the left. This arrangement broadens the mesenteric base, making future volvulus less likely.
4. Appendectomy
An appendectomy is routinely performed during the Ladd procedure. Due to the abnormal position of the cecum and appendix in malrotation, future diagnosis of appendicitis could be delayed or confused. Removal of the appendix prevents this diagnostic dilemma.
5. Inspection and Management of Bowel Viability
The surgeon assesses the bowel for signs of ischemia or necrosis. If non-viable segments are identified, resection and possible creation of an ostomy (stoma) may be necessary.
Postoperative Care
After surgery, patients are closely monitored for signs of infection, continued bowel obstruction, or complications such as short bowel syndrome (if significant resection was required). Initial feeding is typically via intravenous fluids, advancing to oral feeds as bowel function returns. Infants and children generally recover well, with most resuming normal gastrointestinal function within several days.
Outcomes and Prognosis
The prognosis following the Ladd procedure is generally excellent, especially if surgery is performed before bowel necrosis occurs. Most children will lead healthy lives without significant restrictions. However, a minority may experience recurrent symptoms, adhesions, or, rarely, recurrent volvulus.
- Mortality: Mortality rates are low in cases without bowel necrosis, but may increase significantly if volvulus has already caused extensive tissue death by the time of surgery.
- Long-term outcomes: Children may experience mild gastrointestinal symptoms such as intermittent abdominal pain or altered bowel habits, but severe complications are uncommon.
- Recurrence: True recurrence of volvulus after a well-performed Ladd procedure is rare.
Complications
Potential complications of the Ladd procedure include:
- Wound infection or intra-abdominal abscess
- Intestinal obstruction due to postoperative adhesions
- Short bowel syndrome (if extensive resection required)
- Persistent or recurrent abdominal pain
- Rare recurrence of volvulus
Special Considerations
Ladd procedure may be required in older children and adults, often presenting atypically with chronic symptoms such as intermittent abdominal pain, bloating, or failure to thrive. In these cases, diagnosis may be delayed. Minimally invasive approaches are increasingly used, particularly in centers specializing in pediatric surgery.
Nursing Care of a Patient Undergoing Ladd Procedure
Nursing care for a patient undergoing a Ladd procedure is comprehensive and requires attention to perioperative, intraoperative, and postoperative management to ensure optimal outcomes and prevent complications.
Preoperative Nursing Care
Assessment and Preparation
- Comprehensive Assessment: Perform a detailed assessment of the patient’s history, signs and symptoms (such as bilious vomiting, abdominal distension, pain, and feeding intolerance), and review diagnostic findings (e.g., upper GI series, abdominal x-rays).
- Physical Examination: Monitor for signs of acute abdomen, dehydration, electrolyte imbalance, and shock, especially in neonates or infants.
- Laboratory and Diagnostic Review: Ensure results of CBC, electrolytes, blood gases, and imaging studies are available and communicated to the surgical team.
- IV Access and Fluid Management: Establish intravenous access for fluid resuscitation and administration of medications, particularly if the patient is NPO (nil per os, nothing by mouth).
- Gastrointestinal Decompression: Insert a nasogastric tube if ordered, to decompress the stomach and decrease the risk of aspiration or further bowel distension.
- Nutritional Support: Patients are usually kept NPO preoperatively. Monitor nutritional status and prepare for possible parenteral nutrition if fasting is prolonged.
- Infection Control: Administer prophylactic antibiotics as prescribed, and monitor for any signs of infection.
- Patient and Family Education: Educate patient and family about the surgical procedure, expected outcomes, possible risks, and the role of postoperative care. Address any anxieties and offer emotional support.
Intraoperative Nursing Care
Support and Monitoring
- Preparation of the Operating Room: Ensure all necessary surgical equipment and supplies are available, including pediatric-specific instruments if the patient is a child.
- Anesthesia Support: Assist the anesthesiologist in monitoring vital signs and maintaining airway patency, especially in infants and small children.
- Patient Positioning: Properly position the patient to facilitate surgical access and prevent pressure injuries.
- Sterility and Infection Prevention: Maintain strict aseptic technique throughout the procedure to prevent surgical site infection.
- Documentation: Record intraoperative events, vital signs, fluid input/output, blood loss, and any complications.
Postoperative Nursing Care
Immediate Postoperative Care
- Airway, Breathing, Circulation (ABC): Monitor for airway patency, adequate ventilation, and stable circulatory status. Respiratory support may be needed if the patient was under general anesthesia.
- Vital Signs Monitoring: Frequently monitor temperature, heart rate, respiratory rate, and blood pressure for early detection of complications, such as hypovolemic shock, sepsis, or hemorrhage.
- Pain Management: Assess and manage pain using age-appropriate pain scales and multimodal analgesia (IV opioids, acetaminophen, non-pharmacological methods).
- Fluid and Electrolyte Balance: Monitor IV fluids, urine output, and laboratory values to detect and prevent imbalances.
- Gastrointestinal Function: Maintain nasogastric decompression as ordered; monitor for abdominal distension, bowel sounds, passage of flatus or stool, and signs of bowel function return.
- Wound and Surgical Site Care: Inspect the incision for signs of infection, bleeding, or dehiscence. Maintain sterile dressings and reinforce as needed.
- Prevention of Complications:
- Pulmonary complications (e.g., pneumonia, atelectasis)—encourage deep breathing (appropriate to age), repositioning, and early mobilization.
- Venous thromboembolism prevention—use of compression devices and early ambulation as tolerated.
- Monitoring for signs of volvulus, peritonitis, or bowel ischemia (increased pain, tachycardia, distension, absent bowel sounds).
Nutritional Support: Gradual advancement of diet from NPO to clear liquids and then to regular diet as tolerated, following return of bowel function. Monitor for signs of feeding intolerance.
Psychosocial Support: Continue to provide emotional support to the patient and family. Involve child life specialists if appropriate for pediatric patients.
Ongoing Postoperative Care
- Education: Teach the family signs and symptoms of complications, wound care at home, medication administration, and when to seek medical attention.
- Discharge Planning: Collaborate with the medical team, social workers, and case managers to ensure a safe transition to home or rehabilitation. Provide written instructions and resources for follow-up care.
- Follow-Up Appointments: Schedule surgical follow-up to monitor recovery, wound healing, and bowel function.
Potential Complications and Nursing Considerations
- Infection: Monitor for fever, redness, swelling, or discharge at the surgical site. Early detection and prompt intervention are critical.
- Bowel Obstruction: Assess for new-onset vomiting, abdominal distension, or lack of bowel movements, which may indicate obstruction or adhesions.
- Short Bowel Syndrome: Rarely, extensive bowel resection may lead to malabsorption and nutrient deficiencies.
- Psychological Impact: Surgery and hospitalization can be traumatic, especially for children; ongoing support and reassurance are important.
Special Considerations for Pediatric Patients
- Children, especially neonates and infants, require meticulous monitoring due to their limited physiological reserves and unique fluid/electrolyte needs.
- Assessment of pain, hydration, and nutrition must be age-appropriate, using validated tools and family input.
- Parental involvement in care is vital for emotional security and adherence to treatment.
REFERENCES
- Alani M, Rentea RM. Midgut Malrotation. [Updated 2023 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560888/
- American Pediatric Surgical Association. Standardized Toolbox of Education for Pediatric Surgery. APSA Committee of Education 2015-2016. Malrotation. (https://apsapedsurg.org/wp-content/uploads/2020/10/STEPS_Malrotation.pdf)
- Arnaud AP, Supply E, Eaton S, et.al Laparoscopic Ladd’s procedure for malrotation in infants and children is still a controversial approach. https://pubmed.ncbi.nlm.nih.gov/30442460/ J Pediatr Surg. 2019 Sep;54(9):1843-1847.
- Pisano, C., Besner, G.E. (2019). Ladd’s Procedure. In: Papandria, D., Besner, G., Moss, R., Diefenbach, K. (eds) Operative Dictations in Pediatric Surgery. Springer, Cham. https://doi.org/10.1007/978-3-030-24212-1_19
- da Costa KM, Saxena AK. Laparoscopic Ladd Procedure for Malrotation in Newborns and Infants (https://pubmed.ncbi.nlm.nih.gov/32931325/). Am Surg. 2021 Feb;87(2):253-258.
- Frasier LL, Leverson G, Gosain A, et.al. Laparoscopic versus open Ladd’s procedure for intestinal malrotation in adults. https://pubmed.ncbi.nlm.nih.gov/25294535/Surg Endosc. 2015 Jun;29(6):1598-604.
- Mizuta N, Kikuchi T, Fukuda Y. Adult Intestinal Malrotation Treated with Laparoscopic Ladd Procedure. Case Rep Surg. 2022 Oct 18;2022:6874885. doi: 10.1155/2022/6874885. PMID: 36304201; PMCID: PMC9596249.
- Xie W, Li Z, Wang Q, et.al. Laparoscopic vs open Ladd’s procedure for malrotation in neonates and infants: a propensity score matching analysis.https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8793198/. BMC Surg. 2022 Jan 26;22(1):25.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


