


Last Updated on January 21, 2026 by Nurseslab.in Editorial Team
Neobladder reconstruction is a sophisticated surgical procedure that aims to restore urinary function following the removal of the bladder, typically due to bladder cancer or other severe urological conditions. Employing intricate surgical methods and requiring a multidisciplinary approach, neobladder reconstruction offers eligible patients an opportunity to maintain continence and avoid lifelong external urinary diversion, such as an ileal conduit (urostomy bag).
Introduction
The human bladder serves as an essential reservoir, collecting urine produced by the kidneys and providing voluntary control over urination. When the bladder is irreparably damaged or affected by life-threatening disease, its removal—the procedure known as radical cystectomy—becomes necessary. Following cystectomy, reconstructive options include incontinent diversion (ileal conduit), continent cutaneous diversion, and orthotopic neobladder reconstruction. The neobladder, fashioned from a segment of the intestine and connected to the urethra, enables patients to urinate through their native urethra, preserving a semblance of normal urinary function.
Indications for Neobladder Reconstruction
Neobladder reconstruction is most commonly performed following radical cystectomy for muscle-invasive bladder cancer. Other indications include severe neurogenic bladder, congenital anomalies (such as bladder exstrophy), traumatic injury, or chronic inflammatory disease where bladder preservation is impossible.
To be a candidate for neobladder reconstruction, patients generally must:
- Have sufficient renal and hepatic function
- Possess an intact and functional urethra
- Be motivated and able to participate in postoperative rehabilitation
- Not have extensive urethral disease or involvement by cancer
Surgical Techniques
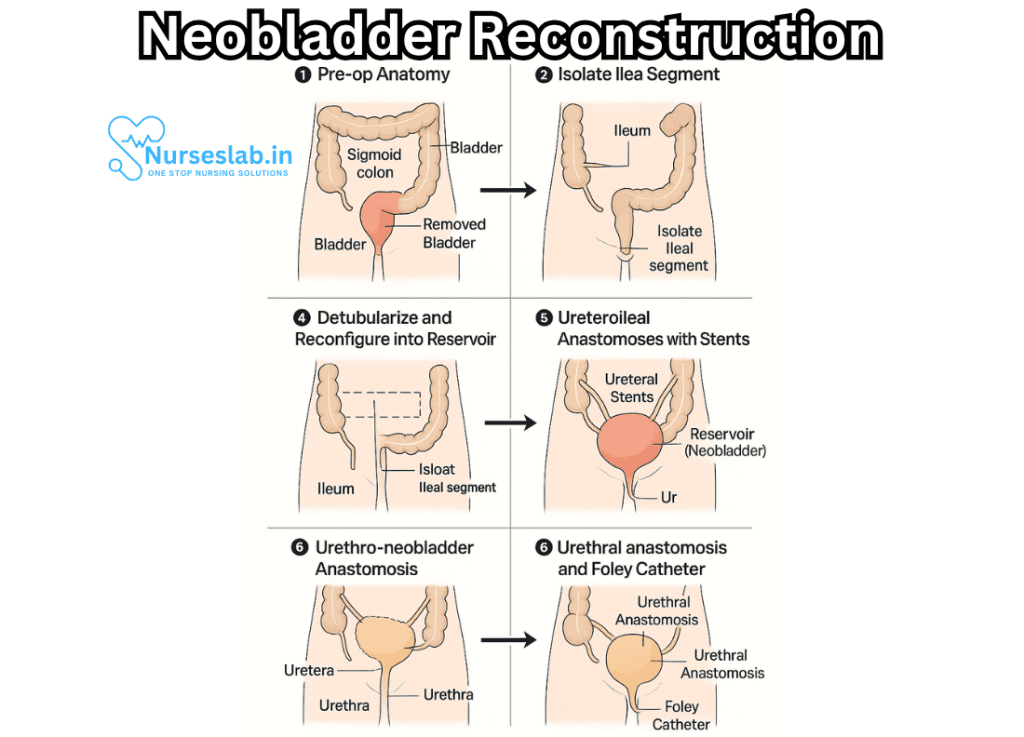
The neobladder is constructed by harvesting a segment of intestine, most commonly the ileum, although the colon or other bowel segments may occasionally be used. The chosen segment is detubularized (opened along its length) and reshaped into a spherical or pouch-like reservoir. This reservoir is then anastomosed (connected) to the urethra, enabling urine to exit via the normal pathway.
Key steps in neobladder reconstruction include:
- Isolation of bowel segment: A portion of the small intestine, typically 40–60 cm, is selected and separated from the bowel, preserving its blood supply.
- Detubularization: The bowel segment is incised along its antimesenteric border and opened to reduce pressure and create a low-pressure reservoir.
- Reservoir formation: The opened bowel is folded and sutured into a spherical or U-shaped pouch, mimicking bladder shape and function.
- Urethral anastomosis: The new reservoir is connected to the urethra, allowing for voluntary urination.
- Ureteral reimplantation: The ureters are implanted into the neobladder through anti-reflux mechanisms to prevent backflow of urine.
- Closure and reconstruction: The surgical field is closed, and drains or catheters may be placed temporarily to promote healing.
There are several named techniques for neobladder construction, including the Studer pouch, Hautmann pouch, and Camey pouch, each utilizing different configurations of bowel tissue and reservoir design.
Perioperative and Postoperative Care
Patients undergoing neobladder reconstruction require meticulous perioperative care. Preoperative assessment includes nutritional optimization, evaluation of renal and hepatic function, and patient education about the procedure and rehabilitation.
Postoperatively, care focuses on:
- Maintaining hydration and electrolyte balance
- Preventing infection and monitoring for leaks
- Ensuring bowel function returns
- Educating the patient on neobladder training
Typically, a urinary catheter remains in place for two to three weeks to allow the anastomosis to heal. Imaging studies are performed before catheter removal to confirm integrity of the neobladder.
Rehabilitation and Adaptation
Rehabilitation after neobladder reconstruction is vital for optimal urinary function. Patients must learn to contract abdominal muscles to initiate voiding, as the neobladder lacks the natural detrusor muscle of the native bladder. Many experience a period of urinary incontinence, particularly at night, which typically improves over several months.
Bladder training includes:
- Scheduled voiding to establish routine emptying
- Pelvic floor exercises to improve continence
- Monitoring fluid intake
- Awareness of signs of incomplete emptying
In some cases, intermittent self-catheterization may be necessary if voiding is inefficient or incomplete.
Complications
Like all major surgical procedures, neobladder reconstruction carries risks. Short-term complications include:
- Infection (urinary tract, wound, or intra-abdominal)
- Anastomotic leak
- Bowel obstruction
- Thromboembolic events
- Bleeding
Long-term complications can include:
- Urinary incontinence (persistent or nocturnal)
- Urinary retention requiring catheterization
- Metabolic disturbances (e.g., acidosis, electrolyte imbalance)
- Neobladder stone formation
- Ureteral stricture or reflux
- Mucus production leading to obstruction
Follow-up care with a urologist is essential to monitor for late complications and ensure the neobladder continues to function effectively.
Outcomes and Quality of Life
Studies demonstrate that, for appropriately selected patients, neobladder reconstruction provides excellent long-term outcomes. Most patients regain significant continence and the ability to void through the urethra. Social confidence, body image, and sexual function often improve compared to incontinent urinary diversion.
Quality of life assessments reveal:
- High satisfaction with urinary continence in daytime
- Variable degrees of nocturnal leakage
- Improvement in body image
- Preservation of sexual function (depending on nerve-sparing technique)
- Need for ongoing surveillance
It is important to note that success depends on patient motivation, physical ability, and regular medical follow-up.
Contraindications and Limitations
Neobladder reconstruction may not be suitable for all patients. Contraindications include:
- Advanced age or poor physical condition
- Severe renal or hepatic dysfunction
- Extensive urethral or pelvic disease
- Previous pelvic radiation affecting bowel or urethra
- Lack of motivation or support for rehabilitation
Alternative urinary diversions may be recommended in these cases.
Nursing Care of Patients with Neobladder Reconstruction
Nursing care is foundational in supporting patients through the perioperative period and their long-term adaptation to a neobladder. This document provides an in-depth overview of best nursing practices, focusing on clinical monitoring, patient education, psychosocial support, and advocacy.
Preoperative Nursing Considerations
- Patient Assessment:
- In-depth physical and psychological assessments are essential. Nurses should review the patient’s medical history, current medications, allergies, baseline renal function, and bowel habits. Screening for risk factors such as malnutrition, infection, and previous abdominal surgeries must be thorough.
- Patient and Family Education:
- Clear communication about the surgical process, expected outcomes, and potential complications is vital. Nurses should provide both verbal and written information, including diagrams or multimedia resources if available, to ensure understanding.
- Informed Consent:
- Support the patient’s autonomy by verifying understanding of the risks, benefits, and alternatives of neobladder reconstruction. Document informed consent and address any questions or concerns compassionately and thoroughly.
- Psychosocial Support:
- Recognise and validate emotional responses, including anxiety or fear. Facilitate contact with support groups, peer mentors, or counselling services as appropriate.
Immediate Postoperative Care
Clinical Vigilance and Monitoring
- Vital Signs:
- Monitor for early signs of shock, infection, bleeding, or sepsis. Frequent checks of blood pressure, pulse, temperature, and oxygen saturation are mandatory, especially in the initial 48 hours after surgery.
- Fluid and Electrolyte Balance:
- Neobladder construction alters urinary physiology. Monitor intake and output meticulously, accounting for urine, wound drainage, and intravenous fluids. Watch for imbalances, especially metabolic acidosis, which may occur due to absorption of urinary solutes through intestinal mucosa.
- Pain Management:
- Assess pain levels regularly and advocate for adequate analgesia. Consider multimodal pain strategies such as epidural analgesia, non-opioid medications, and non-pharmacological interventions (relaxation, guided imagery).
- Surgical Site and Drainage:
- Inspect the abdominal incision, drainage tubes, and surrounding tissues for signs of infection, bleeding, or wound dehiscence. Document all findings and escalate promptly if complications arise.
- Urinary Catheter Care:
- Most patients will have a urethral catheter and possibly suprapubic or stent catheters to facilitate healing and prevent obstruction. Maintain strict aseptic technique, secure catheters adequately, and monitor for patency, leakage, or infection.
Complication Surveillance
- Infection:
- Patients are at increased risk for urinary tract and wound infections. Monitor for fever, dysuria, foul-smelling urine, or purulent wound drainage. Cultures may be necessary if infection is suspected.
- Bleeding:
- Watch for signs of internal or external bleeding, such as tachycardia, hypotension, pallor, or increasing wound drainage. Hematuria is expected initially but should gradually resolve.
- Metabolic Disturbances:
- Monitor for electrolyte imbalances and metabolic acidosis, which may manifest as confusion, nausea, or cardiac arrhythmias.
- Bowel Function:
- The use of bowel tissue can result in temporary or prolonged ileus. Monitor for abdominal distension, lack of bowel sounds, nausea, or vomiting. Early mobilisation and careful advancement of diet are key.
Patient Education and Long-Term Adaptation
Void Training and Continence Management
- Bladder Training:
- Patients must learn to use abdominal muscles (Valsalva manoeuvre) to void, as the neobladder lacks detrusor muscle contractions. Nurses play a crucial role in teaching, supervising, and supporting practice sessions, initially at regular intervals.
- Continence Strategies:
- Discuss the possibility of daytime and nocturnal incontinence, which is most common in the early months. Teach patients about pelvic floor exercises, scheduled voiding, and the use of absorbent products if necessary.
- Monitoring for Retention:
- Teach patients to monitor for incomplete emptying by tracking voided volumes and residuals (using bladder scans if available). Address signs of retention promptly to prevent complications.
Self-Care and Preventing Complications
- Hydration and Diet:
- Advise patients to maintain high fluid intake (unless contraindicated) to prevent mucus plugging and urinary tract infections. Dietary modifications may be necessary to manage metabolic effects.
- Infection Prevention:
- Educate on signs of infection, proper hand hygiene, catheter care, and when to seek medical attention.
- Skin Care:
- Teach strategies for managing skin irritation due to leakage or incontinence, including the use of barrier creams.
- Sexual Health:
- Provide sensitive information about potential sexual dysfunction, options for rehabilitation, and contraception advice if appropriate.
Psychosocial and Ethical Considerations
- Respect for Autonomy and Confidentiality:
- Maintain strict confidentiality and respect for patient preferences regarding care, pain management, and follow-up.
- Emotional Support:
- Recognise body image changes, emotional distress, and the impact on relationships. Facilitate ongoing support from mental health professionals and peer networks.
- Family and Caregiver Involvement:
- Include family members and caregivers in education and discharge planning, respecting the patient’s wishes and privacy.
Discharge Planning and Follow-Up
- Discharge Instructions:
- Provide both verbal and written information about wound care, catheter management, signs of complications, and lifestyle adjustments. Ensure clear instructions for when to seek medical attention.
- Follow-Up Evaluation:
- Arrange for follow-up visits with the surgical team, urologist, and, if needed, metabolic specialists. Monitor kidney function, continence, and overall adaptation to the neobladder.
- Prompt Referral:
- Facilitate referrals to specialty care (wound care, continence nurse, nutritionist, mental health) if healing is delayed or complications arise.
Nursing Advocacy and Holistic Care
Effective nursing care for patients with neobladder reconstruction is anchored in clinical vigilance, patient advocacy, and clear communication. Nurses are instrumental in ensuring optimal recovery, minimising complications, and enhancing patient satisfaction. This involves not only technical expertise but also compassion, education, and respect for individual values and preferences.
REFERENCES
- McAninch JW, et al., eds. Urinary diversions and bladder substitutions. In: Smith & Tanagho’s General Urology. 19th ed. McGraw Hill; 2020. https://accessmedicine.mhmedical.com.
- Chang DT, Lawrentschuk N. Orthotopic Neobladder Reconstruction. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4310095/. Urol Ann. 2015 Jan-Mar;7(1):1-7.
- Qu LG, Lawrentschuk N. Orthotopic Neobladder Reconstruction: Patient Selection And Perspectives. Res Rep Urol. 2019 Dec 11;11:333-341. doi: 10.2147/RRU.S181473. PMID: 31850284; PMCID: PMC6912000.
- Clifford TG, Shah SH, Bazargani ST, et al. Prospective Evaluation of Continence Following Radical Cystectomy and Orthotopic Urinary Diversion Using a Validated Questionnaire. https://pubmed.ncbi.nlm.nih.gov/27256205/. J Urol. 2016;196(6):1685-1691.
- Fasanella D, Marchioni M, Domanico L, et al. Neobladder “Function”: Tips and Tricks for Surgery and Postoperative Management. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9409805/. Life (Basel). 2022 Aug 4;12(8):1193.
- Hobisch A, Tosun K, Kinzl J, et al. Quality of Life after Cystectomy and Orthotopic Neobladder Versus Ileal Conduit Urinary Diversion https://pubmed.ncbi.nlm.nih.gov/11131311/. World J Urol. 2000;18(5):338-344.
- Nouhaud FX, Coughlin G. Advantages of an Intracorporeal W-shaped Neobladder. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8627955/. Eur Urol Open Sci. 2021 Nov 22;35:14-15.
- Sperling CD, et al. Urinary diversion: Core Curriculum 2021. American Journal of Kidney Disease. 2021; doi:10.1053/j.ajkd.2020.12.023.
- Chesnut GT, Rentea RM, Leslie SW. Urinary Diversions and Neobladders. [Updated 2024 May 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560483/
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


