


Understanding Patent Foramen Ovale and Its Closure
PFO closure is a minimally invasive cardiac procedure that seals a persistent opening between the atria to prevent abnormal blood flow and reduce the risk of cryptogenic stroke, using a catheter-delivered device implanted through a vein to permanently close the defect.
Introduction
The human heart, a marvel of biological engineering, is composed of four chambers and operates with remarkable precision throughout a person’s life. Among its many intricacies lies a small, naturally occurring hole between the two upper chambers— the atria— known as the foramen ovale. While this opening is essential during fetal development, in most individuals, it closes shortly after birth. However, in some people, the foramen ovale remains open—a condition known as Patent Foramen Ovale (PFO). For certain patients, particularly those with related health issues, a procedure known as PFO closure may be recommended.
What is Patent Foramen Ovale?
Definition and Anatomy
The foramen ovale is a flap-like opening in the atrial septum (the wall between the right and left atria) that exists naturally during fetal life. It functions as a crucial conduit, allowing oxygen-rich blood from the mother to bypass the non-functioning fetal lungs and flow directly into the left side of the fetal heart. At birth, when the newborn’s lungs assume the role of oxygenating blood, increased pressure in the left atrium pushes the flap of the foramen ovale closed. In the majority of individuals, this closure is permanent, but in approximately 20–25% of adults, the foramen ovale remains at least partially open—hence, Patent Foramen Ovale.
Prevalence
PFO is remarkably common; it is present in one out of every four to five adults. In most cases, a PFO causes no symptoms and is found incidentally during studies for unrelated health concerns.
Why Consider PFO Closure?
Clinical Significance of PFO
While most people with a PFO live without any complications, there are circumstances where its presence can have health implications. The primary reason for considering closure of a PFO is the association between PFO and cryptogenic stroke—a type of stroke with no clearly identifiable cause. In some patients, a blood clot can pass through the PFO from the right side of the heart to the left, then travel to the brain and cause a stroke. This is known as a paradoxical embolism.
Other Conditions Linked to PFO
- Migraine with Aura: Some studies suggest a link between PFO and migraines, particularly migraines with aura, though the evidence remains inconclusive.
- Decompression Illness: Divers are at risk if a PFO allows bubbles formed during rapid ascent to bypass the lungs and enter the arterial circulation.
- Platypnea-Orthodeoxia Syndrome: A rare condition where PFO causes shortness of breath and low oxygen levels when upright.
Indications for Closure
The main indication for PFO closure is to prevent recurrent cryptogenic strokes, particularly in younger patients where no other cause is identified. The decision to proceed with closure is individualized, taking into account the patient’s age, health history, risk factors, and the findings from diagnostic tests.
Diagnostic Evaluation
Diagnosing a PFO involves a combination of clinical assessment and imaging studies. The following are commonly used methods:
- Echocardiogram: An ultrasound of the heart, especially with “bubble study” (injection of agitated saline) to visualize shunt between atria.
- Transesophageal Echocardiography (TEE): Offers higher resolution imaging from within the esophagus and is considered the gold standard for PFO detection.
- Transcranial Doppler Ultrasound: Detects microembolic signals in cerebral arteries, useful in evaluating shunt severity.
PFO Closure: Techniques
Medical vs. Interventional Management
For many years, the only treatment option for patients with a PFO and a history of stroke was medical therapy—typically antiplatelet agents (such as aspirin) or anticoagulants (such as warfarin). Over the last two decades, advances in catheter-based interventions have made percutaneous (through the skin, via a vein) PFO closure a widely accessible option.
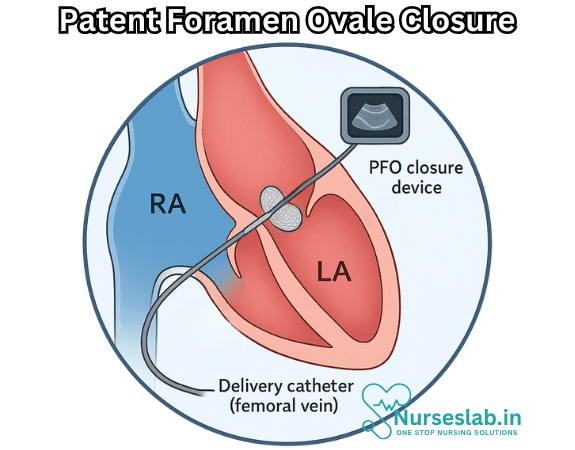
Percutaneous Closure Procedure
The majority of PFO closures are performed in a cardiac catheterization lab under local anesthesia and mild sedation. The procedure steps include:
- Accessing the femoral vein in the groin area with a thin, flexible catheter.
- Guiding the catheter through the venous system into the right atrium of the heart.
- Crossing the PFO using specialized wires and catheters.
- Deploying a closure device (commonly a double-disc device made of metal and fabric) across the PFO, which sandwiches the opening and encourages tissue growth to permanently seal the heart wall.
- Removing the catheters and monitoring the patient in recovery.
Devices Used
Several devices have been approved for PFO closure, including the Amplatzer PFO Occluder, the Gore Cardioform Septal Occluder, and others. The choice of device depends on the patient’s anatomy and physician preference.
Surgical Closure
Surgical closure of PFO is rarely needed and typically reserved for patients undergoing open heart surgery for other reasons.
Benefits and Risks of PFO Closure
Benefits
- Reduces the risk of recurrent cryptogenic stroke in selected patients.
- Minimally invasive with short hospital stays and quick recovery.
- Potentially reduces migraine frequency in some individuals, though evidence is mixed.
Risks
- Device-related complications, such as device migration or embolization (rare).
- Bleeding or vascular complications at the access site.
- Arrhythmias, such as atrial fibrillation, which may occur in a small percentage of patients.
- Allergic or adverse reactions to materials or medications used during the procedure.
Long-term Outcomes
Most patients recover quickly and return to normal activities within days. The heart tissue generally grows over the device within a few months, permanently sealing the PFO. Regular follow-up with echocardiography is recommended to ensure successful closure and monitor for complications.
Current Evidence and Guidelines
Several large clinical trials—such as RESPECT, CLOSE, and REDUCE—have demonstrated that PFO closure can reduce the risk of recurrent stroke in carefully selected patients. Multiple international guidelines now endorse the procedure in specific scenarios, particularly for those under 60 with a history of cryptogenic stroke and no alternate cause.
Controversies and Ongoing Research
While the benefits for recurrent stroke prevention are well established in certain populations, ongoing research continues to investigate:
- The role of PFO closure in migraine management.
- Long-term risks versus benefits in older adults.
- The possibility of PFO closure to prevent decompression illness in divers.
Not all patients with a PFO require closure, and most will never experience related health problems.
Nursing Care of the Patient with PFO Closure
The closure procedure is usually performed percutaneously, utilizing a device that seals the opening. Meticulous nursing care is essential before, during, and after the intervention to ensure patient safety, facilitate recovery, and minimize complications.
Pre-Procedure Nursing Care
- Patient Assessment: Conduct a thorough assessment of the patient’s medical history, including previous cardiovascular events, allergies, medications, and risk factors. Baseline vital signs and relevant laboratory values should be documented.
- Education and Consent: Explain the purpose of the PFO closure, expected outcomes, risks, and benefits. Engage the patient and family in discussion, answer questions, and confirm that informed consent is obtained.
- Preparation: Ensure the patient is NPO (nothing by mouth) for the recommended period prior to the procedure, usually 6-8 hours. Confirm availability of intravenous access and prepare the skin at the insertion site (commonly the femoral vein) according to aseptic technique.
- Medication Management: Review and reconcile current medications, specifically anticoagulants and antiplatelet agents. Collaborate with the medical team regarding adjustments; some agents may need to be withheld or bridged with alternate therapies.
- Psycho-Social Support: Address anxiety and fears by providing emotional support and reassurance. Offer relaxation techniques as needed.
Intra-Procedure Nursing Care
- Patient Monitoring: Continuously monitor vital signs, oxygen saturation, and cardiac rhythm. Watch for signs of adverse reactions to sedation or contrast agents.
- Assistance to the Interventional Team: Ensure sterile technique is maintained and assist with equipment and supply management as needed.
- Safety Precautions: Be vigilant for complications such as arrhythmias, hypotension, or allergic reactions, and respond promptly.
- Documentation: Record procedural events, medications administered, and any deviations from the expected course.
Post-Procedure Nursing Care
- Hemodynamic Monitoring: Observe for changes in vital signs and cardiac rhythm. Monitor for signs of bleeding, hematoma, or vascular compromise at the insertion site.
- Site Care: Inspect the access site for bleeding, swelling, or infection. Maintain a pressure dressing as directed and observe for distal pulse integrity.
- Pain Management: Assess pain level and provide analgesia as appropriate. Monitor for discomfort related to the procedure or access site.
- Anticoagulation and Medication: Administer prescribed antiplatelet therapy, such as aspirin or clopidogrel, which may be continued for several months post-closure. Monitor for side effects or adverse reactions.
- Mobility and Activity: Encourage bed rest for the initial hours post-procedure, particularly if femoral access was used. Gradually reintroduce activity as tolerated, following the physician’s instructions.
- Fluid Balance: Monitor input and output to prevent fluid overload or dehydration. Assess for signs of heart failure, especially in patients with coexisting cardiac conditions.
- Observation for Complications:
- Arrhythmias: Watch for abnormal heart rhythms and report promptly.
- Device-related Issues: Be alert for device embolization, migration, or malfunction.
- Thromboembolic Events: Assess for symptoms of stroke, limb ischemia, or pulmonary embolism.
- Infection: Monitor for fever, chills, or local signs of infection.
Patient and Family Education
- Activity Restrictions: Provide clear guidance on physical limitations, including avoidance of heavy lifting and strenuous exercise during initial recovery.
- Follow-Up Care: Stress the importance of scheduled follow-up appointments for echocardiography and clinical assessment.
- Medication Adherence: Educate on the necessity of taking prescribed antiplatelet therapy as directed, and warn against discontinuation without medical advice.
- Signs and Symptoms to Report: Instruct on recognizing warning signs such as chest pain, shortness of breath, palpitations, sudden neurological changes, or bleeding from the access site.
- Lifestyle and Risk Modification: Discuss strategies for heart health including smoking cessation, balanced diet, regular exercise, and management of comorbidities.
Psychosocial Considerations
- Emotional Support: Recognize the psychological impact of cardiac interventions. Offer resources for counseling and peer support when needed.
- Anxiety Management: Provide reassurance and promote coping strategies to reduce procedural anxiety and facilitate recovery.
- Family Involvement: Encourage family participation in care discussions and education to foster a supportive environment.
Discharge Planning
- Assessment: Ensure the patient is hemodynamically stable and access site is healthy before discharge.
- Written Instructions: Provide comprehensive discharge instructions covering medication, activity, wound care, and emergency contact information.
- Coordination: Arrange for follow-up appointments and communicate with primary care providers as needed.
- Community Resources: Share information on cardiac rehabilitation and support groups available locally.
REFERENCES
- Brown KN, ElBebawy B, Shah AH, et al. Catheter Management of Patent Foramen Ovale. https://pubmed.ncbi.nlm.nih.gov/30725999/. 2023 Mar 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan.
- Carroll JD, Saver JL, Thaler DE, et al. Closure of patent foramen ovale versus medical therapy after cryptogenic stroke. https://pubmed.ncbi.nlm.nih.gov/23514286/. N Engl J Med. 2013 Mar 21;368(12):1092-1100.
- Kent DM, Dahabreh IJ, Ruthazer R, et al. Device Closure of Patent Foramen Ovale after Stroke: Pooled Analysis of Completed Randomized Trials. https://pubmed.ncbi.nlm.nih.gov/26916479/. J Am Coll Cardiol. 2016 Mar 1;67(8):907-917.
- Teshome MK, et al. Patent foramen ovale: A comprehensive review. Current Problems in Cardiology. 2020; doi:10.1016/j.cpcardiol.2018.08.004.
- Patent foramen ovale (PFO). American Heart Association. https://www.heart.org/en/health-topics/congenital-heart-defects/about-congenital-heart-defects/patent-foramen-ovale-pfo.
- Lee DP, Perry SB. Percutaneous Closure of Atrial Septal Defect and Patent Foramen Ovale. In: Samady H, Fearon WF, Yeung AC, King III SB, eds. Interventional Cardiology. 2nd ed. McGraw Hill; 2017.
- MacGrory B, Ohman EM, Feng W, et al. Advances in the management of cardioembolic stroke associated with patent foramen ovale. https://pubmed.ncbi.nlm.nih.gov/35140114/. BMJ. 2022 Feb 9;376:e063161.
- Meier B, Kalesan B, Mattle HP, et al. Percutaneous closure of patent foramen ovale in cryptogenic embolism. https://pubmed.ncbi.nlm.nih.gov/23514285/. N Engl J Med. 2013 Mar 21;368(12):1083-1091.
- Society for Cardiovascular Angiography & Interventions. Patent Foramen Ovale Closure. https://www.secondscount.org/treatment/patent-foramen-ovale-pfo-closure. Last reviewed 11/8/2022.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


