


Introduction
The trachea, commonly referred to as the windpipe, is a vital structure within the human respiratory system. For nurses, a comprehensive understanding of the tracheal anatomy is essential, as it plays a pivotal role in airway management, endotracheal intubation, tracheostomy care, and the assessment and management of respiratory disorders. This document provides an exhaustive exploration of the trachea’s anatomy, focusing on its structure, relations, blood supply, innervation, histology, development, applied anatomy, and clinical significance, tailored for nursing professionals.
Overview of the Trachea
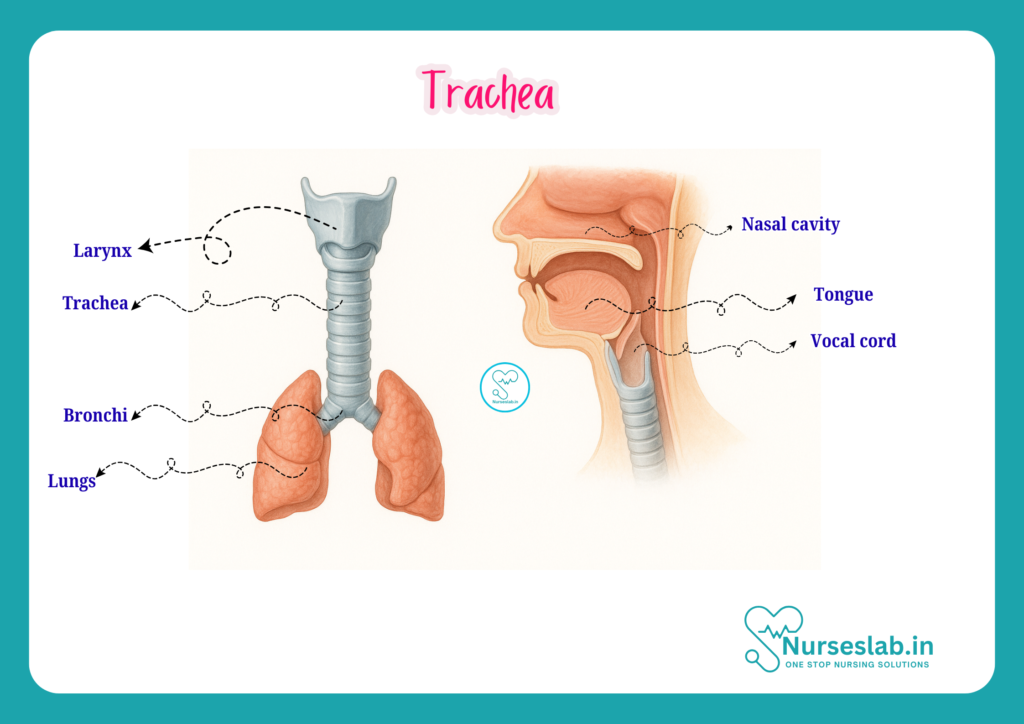
The trachea is a fibrocartilaginous tube that serves as a conduit for air passage between the larynx and the bronchi. It extends from the lower border of the larynx (at the level of the sixth cervical vertebra, C6) to the upper border of the fifth thoracic vertebra (T5), where it bifurcates into the right and left main bronchi. In adults, the trachea measures approximately 10 to 12 cm in length and 2 to 2.5 cm in diameter. The trachea is slightly shorter and wider in males compared to females.
Location and Extent
- Origin: Begins at the lower border of the cricoid cartilage (C6 vertebra).
- Termination: Ends at the level of the sternal angle (T4/T5 intervertebral disc), where it divides into the right and left main bronchi. This point of division is known as the carina.
- Course: The trachea descends anteriorly to the oesophagus in the midline of the neck and upper thorax, entering the superior mediastinum before bifurcating.
External Features and Shape
The trachea is a cylindrical tube that remains open due to the presence of cartilaginous rings. It is slightly flattened posteriorly, where it is related to the oesophagus. The trachea is flexible, allowing movements of the neck and swallowing, but is also strong enough to resist collapse during respiration.
Structural Anatomy
Tracheal Wall Layers
The wall of the trachea consists of four main layers, from inside out:
- Mucosa: The innermost layer, lined by pseudostratified ciliated columnar epithelium containing goblet cells. The cilia help in removing dust and debris, while goblet cells secrete mucus to trap foreign particles.
- Submucosa: Contains connective tissue, blood vessels, nerves, and seromucous glands that further aid in moistening and protecting the respiratory tract.
- Cartilaginous Layer: Composed of 16-20 C-shaped hyaline cartilage rings. These rings are incomplete posteriorly, where the trachealis muscle (smooth muscle) bridges the gap, allowing flexibility and expansion of the oesophagus during swallowing.
- Adventitia: The outermost connective tissue layer that binds the trachea to adjacent structures in the neck and mediastinum.
Tracheal Cartilages
- Each cartilage ring is about 4 mm high and 1 mm thick, with the open part facing posteriorly.
- The rings provide rigidity and prevent collapse, ensuring a patent airway.
- The trachealis muscle and connective tissue complete the posterior wall, allowing changes in tracheal diameter during coughing or forced expiration.
Relations of the Trachea
Cervical Part (Neck)
Anteriorly:
- Skin, superficial fascia, and deep cervical fascia
- Isthmus of the thyroid gland (usually covers the 2nd to 4th tracheal rings)
- Inferior thyroid veins
- Pretracheal lymph nodes
- Sternohyoid and sternothyroid muscles
Posteriorly: Oesophagus
Laterally:
- Lobes of the thyroid gland
- Common carotid arteries
- Recurrent laryngeal nerves
Thoracic Part (Chest)
Anteriorly:
- Manubrium sterni
- Thymus (in children)
- Left brachiocephalic vein
- Aortic arch and its branches (brachiocephalic trunk, left common carotid artery, left subclavian artery)
Posteriorly: Oesophagus (remains posterior throughout)
To the Right: Right lung and pleura, Right vagus nerve, Azygos vein
To the Left: Left lung and pleura, Left recurrent laryngeal nerve, Aortic arch
Blood Supply
The trachea receives its blood supply from different sources in the neck and thorax:
- Upper (Cervical) Part: Supplied by branches of the inferior thyroid arteries (branches of the thyrocervical trunk).
- Lower (Thoracic) Part: Supplied by bronchial arteries (branches of the descending thoracic aorta).
The venous drainage corresponds to the arteries and drains into the inferior thyroid veins and bronchial veins, which ultimately reach the brachiocephalic veins and the azygos system.
Lymphatic Drainage
The lymph from the trachea drains into the pretracheal, paratracheal, and deep cervical lymph nodes. The lower part also communicates with the tracheobronchial lymph nodes near the carina. This lymphatic network is significant in the spread of infections and malignancies.
Nerve Supply
- Parasympathetic: Vagus nerve (cranial nerve X) provides parasympathetic fibres, which are responsible for bronchoconstriction, increased glandular secretion, and cough reflex.
- Sympathetic: Sympathetic fibres originate from the thoracic sympathetic trunk, supplying vasomotor tone and bronchodilation.
- Sensory: Sensory fibres from the vagus nerve mediate the cough reflex and sensation in the tracheal mucosa.
Histology of the Trachea
The tracheal wall, seen under a microscope, reveals several specialised features:
- Mucosa: Lined by pseudostratified ciliated columnar epithelium with goblet cells. The cilia beat upwards, moving mucus and trapped particles towards the pharynx.
- Lamina Propria: Loose connective tissue containing elastic fibres, blood vessels, lymphatics, and immune cells.
- Submucosa: Contains seromucous glands that secrete mucus and serous fluid, aiding in humidification and protection.
- Cartilaginous Layer: C-shaped hyaline cartilage rings, providing structural support.
- Adventitia: Connective tissue layer that merges with surrounding tissues.
Development of the Trachea
The trachea develops during embryogenesis from the foregut. Around the fourth week of intrauterine life, the respiratory diverticulum (lung bud) appears as an outgrowth from the ventral wall of the foregut. This diverticulum elongates and separates from the oesophagus, forming the trachea and later dividing into the bronchial buds. Any abnormal separation can lead to congenital anomalies such as tracheoesophageal fistula or atresia.
Applied Anatomy and Clinical Significance
A thorough knowledge of tracheal anatomy is crucial for nurses in various clinical settings. Below are some key clinical applications:
1.Airway Management
Nurses often assist with airway management, including endotracheal intubation and tracheostomy care. Understanding the anatomical landmarks (such as the cricoid cartilage and the tracheal rings) is vital for correct tube placement and for avoiding injury to the trachea and surrounding structures.
2.Tracheostomy
A tracheostomy is a surgical procedure in which an opening is created in the anterior wall of the trachea, usually between the 2nd and 4th tracheal rings. Nurses must be aware of the structures at risk, such as the thyroid isthmus and inferior thyroid veins, and be proficient in tracheostomy care to prevent complications like infection, bleeding, tracheal stenosis, or tube blockage.
3.Foreign Body Aspiration
The trachea is a common site for foreign body lodgement, especially in children. The right main bronchus is wider, shorter, and more vertical than the left, making the right lung more susceptible to aspirated objects. Nurses must recognise signs of airway obstruction and initiate prompt management.
4.Infections and Inflammation
Tracheitis is an inflammation of the tracheal mucosa, often secondary to viral or bacterial infections. It can lead to airway narrowing, particularly in children (as in croup), necessitating vigilant monitoring and supportive care by nurses.
5.Tumours and Stenosis
Benign or malignant tumours can arise from the tracheal wall. Tracheal stenosis (narrowing) may result from prolonged intubation, trauma, or infection, leading to respiratory distress.
6.Tracheoesophageal Fistula
This congenital anomaly involves an abnormal connection between the trachea and oesophagus, leading to feeding difficulties and recurrent respiratory infections in neonates. Nurses play a crucial role in the pre- and post-operative care of affected infants.
Differences Between Adult and Paediatric Trachea
Understanding the anatomical differences between the adult and paediatric trachea is important for nurses, especially in emergencies:
- Paediatric trachea is shorter, narrower, and more compliant (softer) than in adults.
- The airway is more prone to obstruction from mucus, oedema, or foreign bodies.
- Tracheal rings in infants are less calcified, making the airway more flexible but also more susceptible to dynamic collapse.
- Nurses must use appropriately sized airway devices and exercise extra caution during airway procedures in children.
Common Clinical Procedures Involving the Trachea
- Endotracheal Intubation: Insertion of a tube through the mouth or nose into the trachea to maintain airway patency and allow mechanical ventilation.
- Tracheostomy: Surgical creation of an opening into the trachea; used for prolonged airway support or in cases of upper airway obstruction.
- Bronchoscopy: Visual examination of the trachea and bronchi using a flexible or rigid bronchoscope; helpful for diagnosis and biopsy of lesions.
- Tracheal Suctioning: Removal of secretions from the trachea in patients with artificial airways; requires knowledge of tracheal anatomy to minimise trauma.
Examination and Assessment of the Trachea
- Palpation: The trachea should be centrally located in the neck. Deviation may indicate underlying pathology such as pneumothorax or large mediastinal masses.
- Auscultation: Listening for abnormal breath sounds (stridor, wheeze) can help identify tracheal obstruction or narrowing.
- Imaging: Chest X-ray, CT scan, or MRI can be used to visualise the trachea and detect abnormalities like masses, stenosis, or deviation.
Important Points for Nurses
- Always ensure airway patency in patients with tracheal disorders.
- Monitor for signs of respiratory distress, cyanosis, or stridor.
- Aseptic technique is essential during tracheostomy care and suctioning to prevent infection.
- Be aware of the risk of tracheal injury during airway procedures.
- Educate patients and families about tracheostomy care, signs of complications, and when to seek medical attention.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.



