


Introduction
The human lungs are vital organs at the core of the respiratory system, responsible for the exchange of gases essential to life. Their complex structure and multifaceted functions are of immense interest to medical students, educators, and researchers alike. A thorough understanding of lung anatomy not only forms the foundation for clinical practice but also underpins advances in respiratory medicine and surgery.
Gross Anatomy of the Lungs
External Features
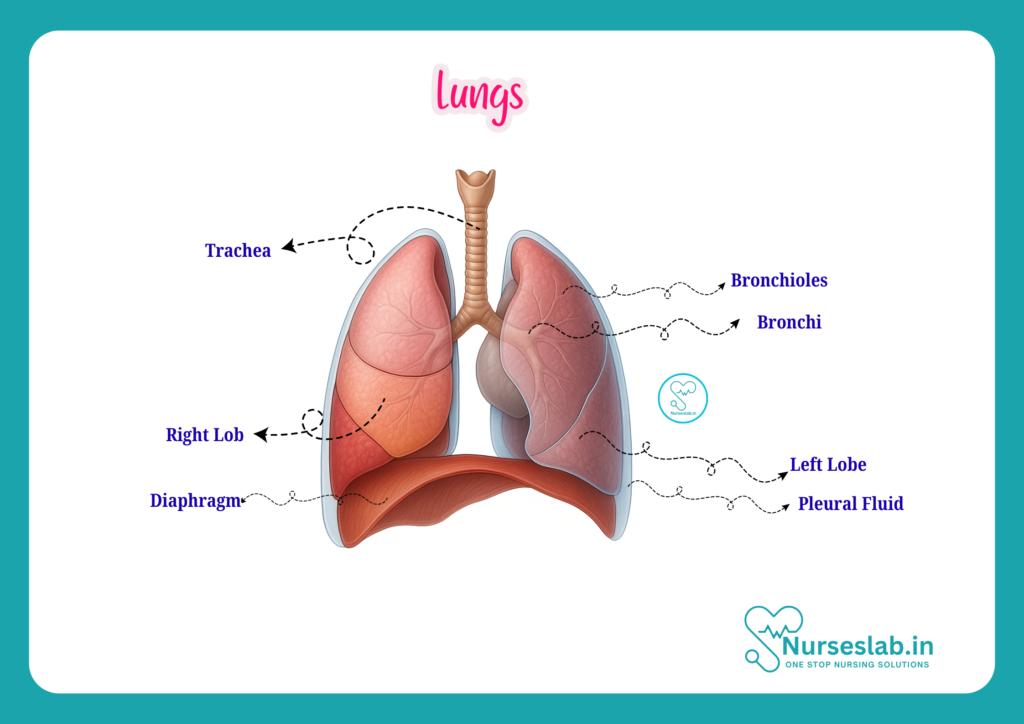
The lungs are paired, spongy organs situated in the thoracic cavity, flanking the mediastinum. Each lung is cone-shaped, with an apex that extends above the level of the first rib and a broad base resting on the diaphragm. The lungs are encased by a double-layered serous membrane called the pleura—comprising the visceral pleura (adhering to the lung surface) and the parietal pleura (lining the thoracic wall). The pleural cavity, a potential space between these layers, contains a small amount of lubricating fluid, facilitating frictionless movement during respiration.
Lobes and Fissures
The right lung is larger and divided into three lobes—superior, middle, and inferior—by the horizontal and oblique fissures. The left lung, slightly smaller due to the cardiac notch accommodating the heart, has two lobes—superior and inferior—separated by an oblique fissure. Each lobe is further subdivided into bronchopulmonary segments, which are functionally and anatomically discrete units.
Surfaces and Borders
Each lung has three distinct surfaces:
- Costal Surface: Faces the ribs and intercostal spaces, smooth and convex.
- Mediastinal Surface: Faces the mediastinum and contains the hilum, through which bronchi, blood vessels, lymphatics, and nerves enter or exit the lung.
- Diaphragmatic Surface: Concave, resting on the dome of the diaphragm.
The anterior and inferior borders are thin and sharp, while the posterior border is rounded and lies adjacent to the vertebral column.
Hilum and Root of the Lung
The hilum is a wedge-shaped area on the mediastinal surface where structures forming the root of the lung enter and leave. The root comprises the primary bronchus, pulmonary artery, pulmonary veins, bronchial arteries and veins, lymphatic vessels, and nerves. The arrangement of these structures differs between the right and left lungs, a detail of clinical importance during surgical procedures.
Microscopic Anatomy
Bronchial Tree
The bronchial tree is a branching system of airways that conducts air from the trachea to the alveoli. It begins with the right and left main bronchi, which enter the lungs at the hilum and divide into lobar (secondary) bronchi—three on the right, two on the left—corresponding to the number of lobes. These further branch into segmental (tertiary) bronchi, each supplying a bronchopulmonary segment. The bronchi continue to branch, forming smaller bronchioles, which lack cartilage and glands, and eventually terminate as terminal bronchioles.
Respiratory Zone: Alveoli and Gas Exchange
The terminal bronchioles give rise to respiratory bronchioles, which possess occasional alveoli in their walls. These lead to alveolar ducts, which open into clusters of alveolar sacs. The alveoli, numbering approximately 300 million in an adult, are thin-walled sacs where the primary exchange of oxygen and carbon dioxide occurs. The walls of alveoli consist of:
- Type I Pneumocytes: Squamous cells forming the majority of the alveolar surface, facilitating gas diffusion.
- Type II Pneumocytes: Cuboidal cells that secrete surfactant, reducing surface tension and preventing alveolar collapse.
- Alveolar Macrophages: Immune cells responsible for phagocytosing debris and pathogens.
The alveolar-capillary barrier, comprising the alveolar epithelium, a fused basement membrane, and capillary endothelium, is remarkably thin (0.2–0.6 micrometres), optimising diffusion.
Interstitial Tissue and Support Structures
The delicate alveolar walls are supported by a fine network of elastic and collagen fibres, providing both resilience and structural integrity. The interstitium contains fibroblasts, mast cells, and a sparse matrix that can become involved in pathological processes such as fibrosis.
Blood Supply of the Lungs
Pulmonary Circulation
The pulmonary arteries carry deoxygenated blood from the right ventricle of the heart to the lungs. Each pulmonary artery divides in accordance with the bronchial tree, ultimately forming a dense capillary network around the alveoli. Here, blood is oxygenated and then returns to the left atrium via the pulmonary veins. This low-pressure system is crucial for efficient gas exchange and is sensitive to changes in oxygen tension, which can induce vasoconstriction in hypoxic areas (hypoxic pulmonary vasoconstriction).
Bronchial Circulation
The bronchial arteries, branches of the thoracic aorta, supply oxygenated blood to the conducting airways, visceral pleura, and supporting tissues of the lung. The bronchial veins drain some of this blood into the azygos and hemiazygos systems, with the remainder joining the pulmonary veins, resulting in a physiological right-to-left shunt.
Nerve Supply of the Lungs
Autonomic Innervation
The lungs receive dual autonomic innervation from the pulmonary plexuses, which contain both sympathetic and parasympathetic fibres:
- Parasympathetic Supply: Derived from the vagus nerve (cranial nerve X), these fibres mediate bronchoconstriction, increased glandular secretion, and vasodilation.
- Sympathetic Supply: Arises from the thoracic sympathetic trunk (T2–T6), causing bronchodilation, decreased mucus secretion, and vasoconstriction.
Sensory fibres relay information about lung stretch, irritation, and pain to the central nervous system, playing a role in reflexes such as coughing and bronchoconstriction.
Lymphatic Drainage
Pathways
Lymphatic vessels in the lung are organised into superficial (subpleural) and deep (peribronchial) networks. The superficial plexus drains the lung surface and visceral pleura, while the deep plexus accompanies the bronchial tree and pulmonary vessels. Lymph ultimately drains to the hilar (bronchopulmonary), tracheobronchial, and paratracheal lymph nodes, before entering the right lymphatic duct or thoracic duct.
Clinical Relevance
Lymphatic drainage plays a vital role in the immune response and the spread of infections or malignancies. Enlargement of hilar or mediastinal nodes may indicate infection, inflammation, or metastatic disease, and is a key consideration in the staging of lung cancer.
Developmental Anatomy
Embryological Origins
Lung development begins in the fourth week of embryogenesis with the formation of the respiratory diverticulum from the ventral wall of the foregut. Subsequent branching morphogenesis gives rise to the bronchial tree, with the alveolar stage continuing postnatally. The key stages include:
- Pseudoglandular Stage (5–16 weeks): Formation of conducting airways.
- Canalicular Stage (16–26 weeks): Development of respiratory bronchioles and vascularisation.
- Saccular Stage (26–36 weeks): Formation of terminal sacs (primitive alveoli).
- Alveolar Stage (36 weeks to 8 years): Maturation and multiplication of alveoli.
Disruptions in this process can result in congenital anomalies such as pulmonary hypoplasia or bronchopulmonary dysplasia.
Functional Aspects
Gas Exchange
The primary function of the lungs is the exchange of oxygen and carbon dioxide between the atmosphere and the bloodstream. Air reaches the alveoli via the conducting airways, and gases diffuse across the thin alveolar-capillary membrane. Oxygen binds to haemoglobin in red blood cells, while carbon dioxide is expelled from the blood into the alveolar air for exhalation. Efficient gas exchange requires a large surface area, thin diffusion barrier, and matching of ventilation (airflow) to perfusion (blood flow).
Mechanics of Breathing
Breathing involves coordinated changes in thoracic volume, driven primarily by the diaphragm and intercostal muscles. During inspiration, contraction of the diaphragm and external intercostals enlarges the thoracic cavity, reducing intrapleural pressure and drawing air into the lungs. Expiration is typically passive, resulting from elastic recoil, but may become active during forceful breathing through the action of abdominal and internal intercostal muscles. The compliance (distensibility) of the lung and chest wall, as well as airway resistance, are important determinants of respiratory mechanics.
Defence Mechanisms
The lungs are equipped with several defence mechanisms to protect against inhaled pathogens and particulates:
- Mucociliary Escalator: Ciliated epithelial cells and mucus-producing goblet cells trap and transport debris out of the airways.
- Alveolar Macrophages: Engulf and digest foreign particles reaching the alveoli.
- Immune Surveillance: Lymphoid tissue in the bronchial walls participates in immune responses.
These mechanisms are vital for maintaining pulmonary health and preventing infection.
Clinical Correlations
Common Diseases
A sound knowledge of lung anatomy is essential for recognising and managing respiratory diseases. Some common conditions include:
- Pneumonia: Infection of the alveoli and interstitium, often visible as consolidation on imaging.
- Chronic Obstructive Pulmonary Disease (COPD): Involves destruction of alveolar walls (emphysema) and airway obstruction (chronic bronchitis).
- Asthma: Reversible bronchoconstriction and airway inflammation, mediated by autonomic nerves and immune cells.
- Lung Cancer: May arise from bronchial epithelium or alveolar cells, with lymphatic spread to regional nodes.
- Pulmonary Embolism: Obstruction of pulmonary arteries by thrombus, impairing gas exchange.
- Interstitial Lung Diseases: Group of disorders causing fibrosis and impaired lung compliance.
Diagnostic Imaging
Imaging modalities such as chest X-ray, computed tomography (CT), and magnetic resonance imaging (MRI) provide detailed visualisation of lung anatomy. Bronchography, ultrasonography, and positron emission tomography (PET) scans are also utilised for specialised indications. Knowledge of normal and variant anatomy is crucial for accurate interpretation of these studies.
Surgical and Procedural Considerations
Surgical interventions, including lobectomy, segmentectomy, and pneumonectomy, require precise anatomical knowledge to avoid injury to vital structures. Bronchoscopy enables direct visualisation and sampling of the bronchial tree, while thoracentesis and pleural biopsies necessitate awareness of pleural reflections and intercostal spaces.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.




