


Understand the structure and function of the alveolus and alveoli, the tiny air sacs in the lungs responsible for gas exchange. Learn how alveoli work, their role in respiration, and how diseases affect alveolar function. Ideal for students, nurses, and medical learners.
Introduction
The alveoli are the cornerstone of the human respiratory system, acting as the primary site for gas exchange between the air we breathe and our bloodstream. For nursing students and healthcare professionals, a thorough understanding of alveolar anatomy and function is essential for effective patient care, especially in respiratory medicine. This article explores the detailed structure and organisation of the alveolus and alveoli, their physiological roles, clinical significance, and implications for nursing practice.
Overview of the Respiratory System
Brief Anatomy
The respiratory system comprises several components that work together to facilitate the exchange of oxygen and carbon dioxide. The primary organs include the nose, pharynx, larynx, trachea, bronchi, bronchioles, and the lungs. The lungs, located within the thoracic cavity, house millions of tiny air sacs called alveoli, which are critical for efficient gas exchange.
Role of the Lungs
The lungs serve as the main site of oxygen uptake and carbon dioxide removal in the body. Air enters through the upper respiratory tract, passes down the trachea, and branches into the bronchi and bronchioles, finally reaching the alveoli. Here, oxygen from inhaled air diffuses into the blood, and carbon dioxide from the blood diffuses out to be exhaled.
Detailed Anatomy of the Alveolus
Structure of the Alveolus
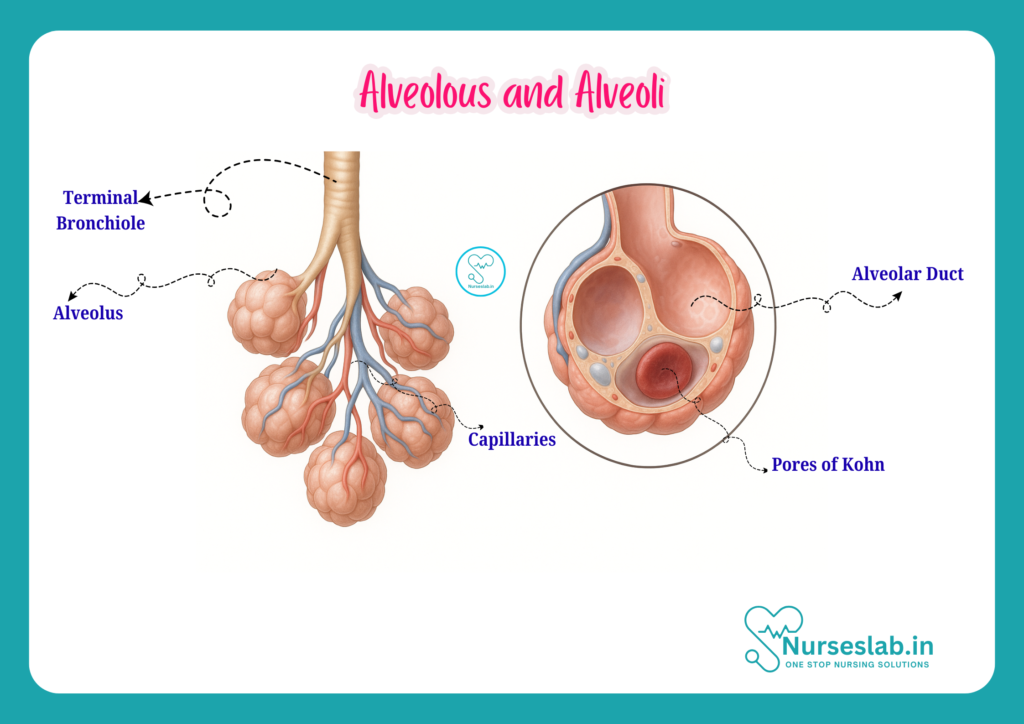
An alveolus (plural: alveoli) is a microscopic, balloon-like structure found at the terminal ends of the respiratory tree. Each alveolus is surrounded by a thin wall, approximately 0.2 micrometres thick, optimising it for rapid gas exchange. These tiny sacs are clustered together like bunches of grapes at the ends of alveolar ducts.
Cell Types in the Alveolus
The alveolar wall consists of several specialised cell types:
- Type I alveolar cells (Type I pneumocytes): These flat, thin cells form the majority of the alveolar surface and are responsible for the actual gas exchange process. They create a minimal barrier for diffusion between alveolar air and capillary blood.
- Type II alveolar cells (Type II pneumocytes): These cuboidal cells are fewer in number but essential for producing surfactant, a substance that reduces surface tension within the alveolus, preventing its collapse during exhalation. Type II cells also play a role in alveolar repair.
- Alveolar macrophages: These immune cells patrol the alveolar surface, engulfing and removing dust, bacteria, and other foreign particles, thus maintaining a sterile environment.
- Capillary endothelial cells: These line the blood vessels surrounding the alveoli and participate in the gas exchange process.
Blood Supply to the Alveoli
Each alveolus is richly supplied by a network of pulmonary capillaries. The pulmonary artery delivers deoxygenated blood from the right ventricle of the heart to the lungs, where it branches extensively into smaller vessels, eventually forming a dense capillary bed around the alveoli. Oxygen diffuses from the alveolar air into the blood, while carbon dioxide moves in the opposite direction. The oxygenated blood then returns to the left atrium of the heart via the pulmonary veins.
Histological Features
Under the microscope, the alveolar wall appears as a delicate, thin membrane composed of the alveolar epithelium, a basement membrane, and the capillary endothelium. The three layers together form the respiratory membrane, which is the actual site of gas exchange. The thinness of this membrane (often less than 0.5 micrometres) allows for rapid diffusion of respiratory gases.
Alveoli as a Collective Unit
Organisation and Distribution in the Lungs
Alveoli are not isolated structures; they are organised into clusters called alveolar sacs at the ends of alveolar ducts. Each lung contains approximately 300 million alveoli, providing a total surface area of about 70 square metres — roughly the size of a tennis court. This vast surface area is crucial for meeting the body’s oxygen demands.
Numbers and Variation
The number of alveoli can vary with age, genetic factors, and environmental influences. At birth, the lungs contain around 20–50 million alveoli, which increase in number and size as the child grows, reaching adult levels by late adolescence.
Physiological Functions of the Alveoli
Gas Exchange
The primary function of the alveoli is to facilitate gas exchange. Oxygen in inhaled air diffuses across the thin alveolar membrane into the blood, while carbon dioxide diffuses from the blood into the alveolar space to be exhaled. This process is driven by differences in partial pressure of gases on either side of the respiratory membrane (a concept known as diffusion gradient).
Surfactant Production
Type II alveolar cells secrete surfactant, a mixture of phospholipids and proteins. Surfactant reduces the surface tension of the alveolar fluid, preventing collapse of the alveolus during exhalation and ensuring stability across varying lung volumes. This substance is particularly crucial in the neonatal period, as insufficient surfactant can lead to respiratory distress syndrome in premature infants.
Diffusion Mechanisms
Gas exchange in the alveoli occurs via passive diffusion, governed by Fick’s Law. The rate of diffusion depends on:
- The surface area available for exchange (high in healthy lungs)
- The thickness of the respiratory membrane (normally very thin)
- The partial pressure difference of gases
- The solubility of the gases in the membrane
Any condition that reduces surface area, increases membrane thickness, or alters pressure gradients can impair gas exchange and result in clinical symptoms.
Clinical Relevance
Common Diseases Affecting the Alveoli
- Pneumonia: Infection and inflammation of the alveoli lead to accumulation of fluid and pus, reducing effective gas exchange and causing symptoms like breathlessness, fever, and cough. In severe cases, it can result in respiratory failure.
- Emphysema: A type of chronic obstructive pulmonary disease (COPD), emphysema involves the destruction of alveolar walls, leading to larger, less efficient air spaces, decreased surface area for gas exchange, and persistent shortness of breath.
- Pulmonary oedema: Accumulation of fluid in the alveoli impairs oxygen diffusion, commonly seen in heart failure.
- Acute Respiratory Distress Syndrome (ARDS): This severe condition is characterised by widespread alveolar damage, increased membrane permeability, and impaired oxygenation.
- Interstitial lung diseases: These conditions cause scarring (fibrosis) of lung tissue, thickening the alveolar membrane and reducing gas exchange efficiency.
Nursing Assessment and Patient Care Considerations
Nurses play a vital role in the assessment and management of patients with alveolar disorders. Key responsibilities include:
- Monitoring respiratory rate, depth, and effort
- Assessing oxygen saturation (SpO2) using pulse oximetry
- Observing for signs of respiratory distress, such as cyanosis, tachypnoea, and use of accessory muscles
- Administering oxygen therapy as prescribed
- Ensuring airway patency and assisting with sputum clearance
- Educating patients and families about respiratory care and disease prevention
Early recognition and intervention can prevent complications and improve patient outcomes. Nurses should also be familiar with infection control practices, particularly in conditions like pneumonia and tuberculosis, to prevent transmission within healthcare settings.
Development and Ageing of the Alveoli
Alveolar Development
Alveolar development begins in the foetal period and continues through early childhood. During gestation, simple sac-like structures form, gradually branching and subdividing to create the mature alveolar architecture. The production of surfactant begins around the 24th week of gestation, reaching sufficient levels by about 34–36 weeks.
Changes with Age
With ageing, several changes occur in the alveolar structure:
- Loss of elastic tissue, resulting in decreased lung compliance and reduced efficiency of gas exchange
- Gradual enlargement of alveolar spaces, similar to mild emphysema
- Decreased number and function of cilia, increasing susceptibility to infection
- Reduced capacity for alveolar repair and regeneration
These changes contribute to the increased risk of respiratory illnesses and decreased exercise tolerance in elderly individuals.
Diagnostic and Therapeutic Implications
Imaging and Assessment
Several diagnostic tools are available to assess alveolar health and function:
- Chest X-ray: Commonly used to detect pneumonia, pulmonary oedema, and other alveolar pathologies.
- Computed Tomography (CT) scan: Provides detailed images of lung parenchyma, useful for diagnosing interstitial lung diseases and emphysema.
- Pulmonary function tests (PFTs): Measure lung volumes, capacities, and gas exchange efficiency.
- Arterial blood gas (ABG) analysis: Assesses levels of oxygen and carbon dioxide in the blood, indicating the effectiveness of alveolar gas exchange.
Therapeutic Interventions
Management of alveolar diseases may include:
- Oxygen therapy to address hypoxaemia
- Antibiotics for infections such as pneumonia
- Bronchodilators and steroids for inflammatory conditions
- Physiotherapy to enhance sputum clearance and improve ventilation
- Mechanical ventilation in severe respiratory failure
Nursing Roles in Diagnostics and Interventions
Nurses are integral to the diagnostic and therapeutic process, responsible for:
- Preparing patients for imaging or procedures
- Monitoring for adverse reactions
- Assisting with respiratory therapies
- Educating patients on medication adherence and lifestyle modification
- Coordinating multidisciplinary care and follow-up
Summary and Key Takeaways
– The alveolus is the fundamental unit of the lung, optimised for rapid and efficient gas exchange.
– Alveoli are composed of specialised cells, including Type I and II pneumocytes and alveolar macrophages, each with unique and vital functions.
– Clinical conditions affecting the alveoli, such as pneumonia and emphysema, can significantly impair respiratory function and require prompt nursing assessment and intervention.
– Alveolar development begins in utero and continues through childhood, while ageing brings structural and functional changes that impact respiratory health.
– Nurses play a crucial role in the detection, management, and education of patients with alveolar disorders, ensuring better outcomes through holistic care.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.



