


Last Updated on July 7, 2026 by Nurseslab.in Editorial Team
Introduction
Understanding the anatomy of spinal nerves is essential for nurses in all areas of practice. Spinal nerves are critical components of the peripheral nervous system and play a significant role in transmitting sensory and motor information between the body and the brain. For nurses, a thorough knowledge of spinal nerve anatomy aids in accurate patient assessment, recognition of neurological disorders, and effective care planning.
Overview of the Nervous System: Central and Peripheral Divisions
The nervous system is responsible for coordinating all bodily functions and responses to internal and external stimuli. It is divided into two main parts:
- Central Nervous System (CNS): Comprises the brain and spinal cord. It processes information and issues commands.
- Peripheral Nervous System (PNS): Consists of all the nerves outside the CNS, including cranial and spinal nerves. It transmits signals between the CNS and the rest of the body.
Spinal nerves are a key component of the PNS. They facilitate communication between the spinal cord and peripheral organs, muscles, and skin.
Spinal Nerves: Definition and General Features
Spinal nerves are mixed nerves that arise from the spinal cord. Each spinal nerve connects the central nervous system to specific regions of the body. There are 31 pairs of spinal nerves in the human body. These nerves are named and numbered according to the region of the vertebral column from which they emerge.
- Each spinal nerve is formed by the joining of a dorsal (posterior) root and a ventral (anterior) root.
- Spinal nerves are “mixed” because they carry both sensory (afferent) and motor (efferent) fibres.
- They exit the vertebral column through openings called intervertebral foramina.
Anatomical Structure: Roots, Ganglia, and Branches
The anatomy of spinal nerves is complex but can be simplified into three main parts: roots, ganglia, and branches.
Roots
- Dorsal (Posterior) Root: Contains sensory nerve fibres. These fibres carry information from the body to the spinal cord.
- Ventral (Anterior) Root: Contains motor nerve fibres. These fibres transmit signals from the spinal cord to muscles and glands.
Ganglia
The dorsal root has an enlargement called the dorsal root ganglion. This ganglion contains the cell bodies of sensory neurons. There is no corresponding ganglion in the ventral root.
Branches (Rami)
After emerging from the intervertebral foramen, each spinal nerve divides into several branches called rami:
- Dorsal (Posterior) Ramus: Supplies muscles and skin of the back.
- Ventral (Anterior) Ramus: Supplies muscles and skin of the limbs and the anterior trunk. It forms nerve plexuses in certain regions.
- Meningeal Branch: Re-enters the vertebral canal to supply the meninges and blood vessels of the spinal cord.
- Rami Communicantes: Connect the spinal nerves to the sympathetic chain of the autonomic nervous system.
Classification of Spinal Nerves
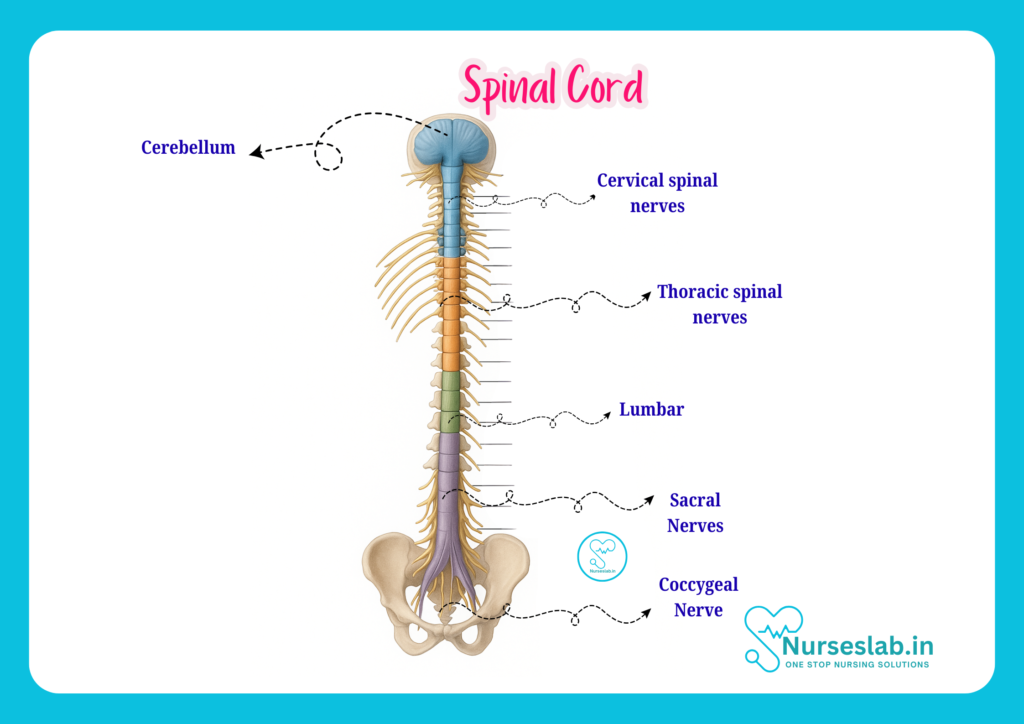
The 31 pairs of spinal nerves are classified based on their location along the vertebral column:
- Cervical Nerves (C1-C8): 8 pairs
- Thoracic Nerves (T1-T12): 12 pairs
- Lumbar Nerves (L1-L5): 5 pairs
- Sacral Nerves (S1-S5): 5 pairs
- Coccygeal Nerve (Co1): 1 pair
Each group of nerves serves specific regions of the body. The naming corresponds to the vertebrae above or below which they exit.
Cervical Spinal Nerves (C1-C8)
There are 8 pairs of cervical nerves, although there are only 7 cervical vertebrae. The first cervical nerve emerges above the atlas (C1), and the eighth emerges below the seventh cervical vertebra.
Thoracic Spinal Nerves (T1-T12)
Twelve pairs correspond to the twelve thoracic vertebrae. These nerves primarily serve the chest and upper abdominal wall.
Lumbar Spinal Nerves (L1-L5)
Five pairs emerge from the lumbar region, supplying the lower back and parts of the lower limbs.
Sacral Spinal Nerves (S1-S5)
Five pairs arise from the sacral region, innervating the pelvic organs and lower limbs.
Coccygeal Spinal Nerve (Co1)
A single pair arises from the coccyx, contributing to innervation of the skin around the coccygeal region.
Functional Aspects: Sensory and Motor Functions
Spinal nerves perform both sensory and motor functions, making them crucial for normal body movement and perception.
Sensory (Afferent) Functions
Sensory fibres carry information from receptors in the skin, muscles, and joints to the spinal cord. This includes sensations such as touch, pain, temperature, and proprioception (awareness of body position).
Motor (Efferent) Functions
Motor fibres transmit impulses from the spinal cord to muscles and glands. This enables voluntary movements and involuntary responses (reflexes).
Reflex Arcs
Spinal nerves play a central role in reflex actions. A reflex arc involves a direct pathway from sensory input to motor output via the spinal cord, often without involving the brain. This allows for quick, automatic responses to certain stimuli, such as pulling your hand away from a hot object.
Major Plexuses: Cervical, Brachial, Lumbar, and Sacral Plexuses
Except for the thoracic spinal nerves, the ventral rami of spinal nerves join to form networks called plexuses. These plexuses enable nerve fibres to be redistributed, so that each peripheral nerve contains fibres from multiple spinal nerves.
Cervical Plexus (C1-C4)
The cervical plexus lies deep in the neck. It supplies the skin and muscles of the neck, parts of the head, and shoulders. The most important nerve from this plexus is the phrenic nerve, which controls the diaphragm and is crucial for breathing.
Brachial Plexus (C5-T1)
Located in the shoulder region, the brachial plexus supplies the upper limb. Major nerves from this plexus include the radial nerve, median nerve, and ulnar nerve. Injuries to this plexus can lead to weakness or paralysis of the arm.
Lumbar Plexus (L1-L4)
The lumbar plexus is found in the lower back. It innervates the anterior and medial thigh. The femoral nerve and obturator nerve are the main branches, controlling thigh muscles and sensation.
Sacral Plexus (L4-S4)
This plexus lies in the pelvis and supplies the buttocks, posterior thigh, and all of the leg and foot. The largest nerve from this plexus is the sciatic nerve, the longest and thickest nerve in the body.
Clinical Relevance:
A sound understanding of spinal nerve anatomy is vital for identifying and managing various clinical conditions. Nurses often encounter patients with nerve injuries, compressions, or infections affecting spinal nerves.
Common Disorders and Injuries
- Herniated Disc: Displacement of the intervertebral disc can compress spinal nerves, causing pain, numbness, or weakness.
- Radiculopathy: Irritation or injury to a spinal nerve root, leading to radiating pain and sensory changes along the nerve’s distribution.
- Sciatica: Compression or inflammation of the sciatic nerve, resulting in pain radiating down the leg.
- Peripheral Neuropathy: Damage to peripheral nerves, including spinal nerves, causing tingling, weakness, or loss of sensation.
- Shingles (Herpes Zoster): Reactivation of the varicella-zoster virus in a spinal nerve, producing painful skin rashes along the affected dermatome.
- Brachial Plexus Injury: Trauma to the brachial plexus affecting arm and hand function.
- Cauda Equina Syndrome: Compression of nerves in the lower spinal canal, an emergency requiring immediate intervention.
Nursing Considerations
- Early identification of neurological signs and symptoms, such as muscle weakness, sensory loss, or changes in reflexes, is crucial.
- Regular monitoring of patients at risk of nerve injury, especially after trauma or surgery involving the spine.
- Patient education on posture, safe movement, and prevention of nerve injuries.
- Providing support and reassurance to patients experiencing chronic pain or disability due to nerve disorders.
- Prompt referral to medical professionals for advanced management when necessary.
Implications of Spinal Nerve Injury
Injuries to spinal nerves can lead to loss of function in the areas supplied by the affected nerve. The extent of disability depends on the location and severity of the injury. For example:
- Cervical Nerve Injury: May affect breathing, arm movement, and sensation.
- Thoracic Nerve Injury: May impact trunk control and abdominal muscles.
- Lumbar/Sacral Nerve Injury: Can result in weakness or paralysis of the legs, and loss of bladder or bowel control.
Prompt recognition and intervention can prevent complications and improve patient outcomes.
Assessment and Care: Techniques for Evaluating Spinal Nerve Function
Nurses play a vital role in assessing spinal nerve function and identifying abnormalities. The following techniques are commonly used:
History Taking
- Ask about onset, duration, and character of symptoms such as pain, numbness, or weakness.
- Inquire about recent injuries, infections, or medical conditions affecting the nervous system.
Physical Examination
- Inspection: Observe for muscle wasting, abnormal posture, or involuntary movements.
- Palpation: Feel for tenderness or swelling along the spine and limbs.
- Motor Testing: Assess muscle strength in different groups supplied by various spinal nerves.
- Sensory Testing: Evaluate touch, pain, temperature, and vibration sense in areas supplied by specific nerves (dermatomes).
- Reflex Testing: Check deep tendon reflexes (e.g., knee-jerk, ankle-jerk) to assess nerve integrity.
Special Tests
- Straight Leg Raise: Used to assess sciatic nerve irritation.
- Tinel’s Sign: Tapping over a nerve to elicit tingling, indicating nerve irritation.
Documentation and Reporting
- Document findings accurately and report any significant changes to the healthcare team.
- Use standard neurological assessment tools and charts for consistent monitoring.
Care Planning
- Develop care plans based on the patient’s functional status and needs.
- Coordinate with physiotherapists, occupational therapists, and doctors for rehabilitation and management.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.



