


The study of thoracic anatomy is integral to nursing practice, underpinning many aspects of patient care, especially in respiratory and cardiovascular health. Clear understanding of these structures equips nurses to assess, monitor, and intervene effectively in diverse clinical scenarios, from routine care to emergencies.
Introduction: Importance of Thoracic Anatomy in Nursing Practice
Nurses are often at the frontline of patient assessment, management, and education. Knowledge of thoracic anatomy is crucial in interpreting respiratory movements, understanding the mechanics of breathing, and recognising signs of distress or disease. Whether monitoring patients with respiratory illnesses, assisting in procedures, or providing post-operative care, a sound grasp of the diaphragm, intercostal muscles, and thoracic cage forms the foundation for safe and effective nursing interventions.
Section 1: Anatomy of the Diaphragm
Structure and Attachments
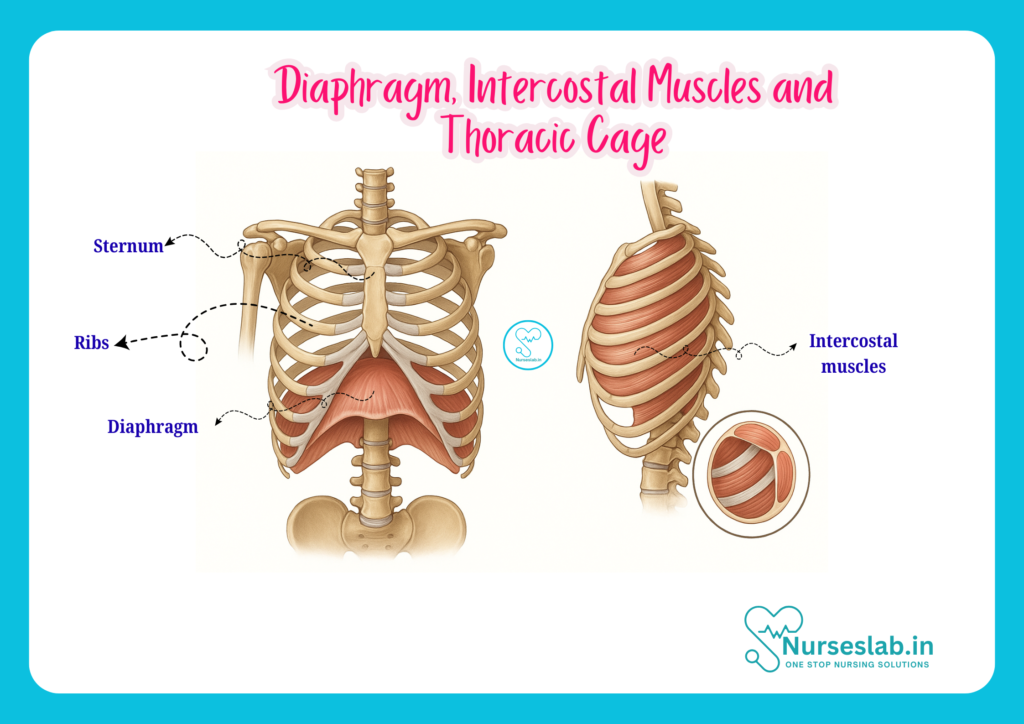
The diaphragm is a dome-shaped, musculotendinous partition that separates the thoracic cavity from the abdominal cavity. It is the principal muscle of respiration. Structurally, the diaphragm consists of a central tendinous part and a peripheral muscular part. The muscular portion is further divided into three sections based on origin:
- Sternal part: Originates from the posterior surface of the xiphoid process.
- Costal part: Arises from the inner surfaces of the lower six ribs and their costal cartilages.
- Vertebral part: Emerges from the lumbar vertebrae via two crura (right and left) and arcuate ligaments.
The diaphragm’s shape resembles two domes, with the right dome typically higher than the left due to the presence of the liver beneath it.
Openings of the Diaphragm
Several important structures pass through the diaphragm via three major openings:
- Caval opening (T8): Located in the central tendon, allows passage of the inferior vena cava and right phrenic nerve.
- Oesophageal hiatus (T10): In the muscular part, transmits the oesophagus, vagus nerves, and oesophageal branches of left gastric vessels.
- Aortic hiatus (T12): Behind the diaphragm, for the aorta, thoracic duct, and azygos vein.
Other minor openings accommodate nerves and vessels, including the sympathetic trunks and splanchnic nerves.
Nerve Supply
The diaphragm receives motor innervation primarily from the phrenic nerve (roots C3, C4, and C5), which also carries sensory fibres to the central tendon. Peripheral portions are supplied by lower intercostal nerves (T5-T12). The mnemonic “C3, 4, 5 keep the diaphragm alive” is often used to remember the phrenic nerve’s contribution.
Blood Supply
The diaphragm’s arterial supply includes:
- Superior surface: Pericardiacophrenic and musculophrenic arteries (branches of the internal thoracic artery), and superior phrenic arteries (branches of the thoracic aorta).
- Inferior surface: Inferior phrenic arteries (branches of the abdominal aorta).
Venous drainage mirrors arterial supply, with veins draining into the brachiocephalic, azygos, and abdominal veins.
Functions of the Diaphragm
The diaphragm is the primary muscle of inspiration. On contraction, it flattens and descends, increasing thoracic volume and reducing intra-thoracic pressure, drawing air into the lungs. During expiration, it relaxes and ascends, aiding passive expulsion of air. Additionally, the diaphragm assists in expulsive activities such as coughing, sneezing, vomiting, defaecation, and childbirth by increasing intra-abdominal pressure.
Clinical Significance
Diaphragmatic dysfunction can result from trauma, surgery, neuropathy, or disease, leading to respiratory compromise. Paralysis, often due to phrenic nerve injury, manifests as paradoxical movement of the affected hemidiaphragm. Hiatal hernia, where abdominal contents herniate through the oesophageal hiatus, is another common clinical issue. Nurses must be vigilant for signs of respiratory distress, impaired cough reflex, or post-operative complications related to diaphragmatic impairment.
Section 2: Intercostal Muscles
Types of Intercostal Muscles
The intercostal muscles occupy the spaces between the ribs and play a vital role in the mechanics of breathing. There are three layers:
- External intercostal muscles: The outermost layer, fibres run inferomedially (downwards and forwards), akin to putting hands in pockets.
- Internal intercostal muscles: Middle layer, fibres run inferolaterally (downwards and backwards), perpendicular to the external layer.
- Innermost intercostal muscles: The deepest layer, with fibres paralleling the internal intercostals, separated by neurovascular bundles.
Origin and Insertion
- External intercostals: From the lower border of the rib above to the upper border of the rib below, extending from the tubercles posteriorly to the costochondral junctions anteriorly.
- Internal intercostals: From the lateral edge of the costal groove of the rib above to the upper border of the rib below, extending from sternum anteriorly to the angles of the ribs posteriorly.
- Innermost intercostals: Occupy the lateralmost part of the intercostal space, divided into subcostal and transversus thoracis groups.
Nerve and Blood Supply
All intercostal muscles are supplied by the intercostal nerves (ventral rami of T1-T11). The corresponding intercostal arteries and veins, running in the costal grooves, supply blood. The neurovascular bundle (vein, artery, nerve – VAN) lies between the internal and innermost intercostals, protected by the rib above.
Functions
The intercostal muscles stabilise the thoracic wall and facilitate breathing:
- External intercostals: Elevate ribs during inspiration, increasing thoracic volume.
- Internal intercostals: Depress ribs during forced expiration, decreasing thoracic volume.
- Innermost intercostals: Assist internal intercostals in forced expiration.
Their coordinated action is essential for effective ventilation and maintenance of negative intra-thoracic pressure.
Clinical Notes
Intercostal muscle dysfunction may present in conditions such as rib fractures, thoracic surgery, or neuromuscular diseases. Intercostal nerve injury can lead to pain, impaired breathing, or altered sensation. Nurses should monitor for signs of respiratory difficulty, pain on inspiration, or abnormal chest movements, especially post-trauma or surgery.
Section 3: Thoracic Cage
Bones of the Thoracic Cage
The thoracic cage, commonly called the rib cage, provides a protective enclosure for the heart, lungs, and major vessels. It consists of:
- Ribs: Twelve pairs. True ribs (1-7) attach directly to the sternum via costal cartilages. False ribs (8-10) attach indirectly, while floating ribs (11-12) have no anterior attachment.
- Sternum: A flat bone comprising three parts: manubrium (superior), body (middle), and xiphoid process (inferior).
- Thoracic vertebrae: Twelve vertebrae (T1-T12) form the posterior boundary, articulating with the ribs.
Joints and Ligaments
The thoracic cage’s mobility and stability are enabled by various joints and ligaments:
- Costovertebral joints: Between rib heads and vertebral bodies, allowing elevation and depression during breathing.
- Costotransverse joints: Between rib tubercles and transverse processes of vertebrae.
- Sternocostal joints: Between costal cartilages and sternum.
- Interchondral joints: Between costal cartilages of ribs 8-10.
- Ligaments: Costotransverse, radiate, and intra-articular ligaments reinforce joints, preventing dislocation.
Overall Structure and Functions
The thoracic cage is conical, wider at the base, and flattened anteriorly and posteriorly. Its primary functions are:
- Protection: Shields vital organs (heart, lungs, major vessels) from trauma.
- Support: Provides attachment points for muscles involved in respiration, posture, and upper limb movement.
- Breathing mechanics: Expands and contracts to facilitate ventilation.
The flexibility of the thoracic cage allows for changes in volume during respiration, while its rigidity maintains structural integrity.
Section 4: Integration and Clinical Relevance
Breathing Mechanics
Normal respiration involves coordinated movement of the diaphragm, intercostal muscles, and thoracic cage. During inspiration, the diaphragm contracts and descends, while the external intercostals elevate the ribs, expanding the chest cavity. Expiration is typically passive, with relaxation of these muscles, but becomes active during exertion or respiratory distress, engaging the internal and innermost intercostals.
Common Pathologies
Several conditions affect these thoracic structures:
- Diaphragmatic paralysis: Often due to phrenic nerve injury, leading to impaired ventilation.
- Rib fractures: Cause pain, restrict movement, and may damage underlying organs.
- Pneumothorax: Air in the pleural cavity, often due to trauma, disrupts normal breathing mechanics.
- Intercostal neuralgia: Nerve injury or inflammation presents as pain along the rib cage.
- Thoracic deformities: Conditions like scoliosis or pectus excavatum alter thoracic mechanics and may compromise respiratory function.
- Hiatal hernia: Abdominal viscera herniate through the diaphragm, affecting digestion and sometimes respiration.
Implications for Nursing Care
Nurses should be adept at assessing thoracic movement, respiratory rate, and pattern. Recognising abnormal chest expansion, use of accessory muscles, or paradoxical movements is vital for early intervention. Pain management, respiratory exercises, and monitoring for complications (e.g., hypoxia, infection) are essential in post-thoracic surgery or trauma care. Understanding thoracic anatomy also assists in procedures such as chest tube insertion, cardiopulmonary resuscitation, and positioning patients to optimise ventilation.
Section 5: Summary and Key Points
- The diaphragm is the primary muscle of respiration, with important roles in breathing and intra-abdominal pressure regulation.
- Intercostal muscles stabilise the chest wall and facilitate both inspiration and expiration.
- The thoracic cage protects vital organs, supports respiratory movements, and provides muscle attachment points.
- Clinical conditions affecting these structures can significantly impact breathing and overall patient health.
- Nurses must integrate anatomical knowledge with clinical skills to assess, identify, and manage thoracic pathology effectively.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.



