


Last Updated on November 20, 2025 by Nurseslab.in Editorial Team
Safety: Accidents and injuries are the leading causes of death among young men, while suffocation is the most common cause of death among infants. Drowning deaths are most common in toddlers. Additional causes of unintentional injuries include motor vehicle accidents, poisoning, drug overdoses, burns, and falls.
The following are the risk factors that increase the patient’s risk for injury:
Individual factors:
- Neuromuscular impairments that may cause decreased muscle strength and alteration in gait and balance
- Extremes in age (very young or very old)
- Perceptual disturbances
- Chronic debilitating illnesses
- Nonadherence with safety protocols
- Recent physical trauma
- Low socioeconomic status
- Smoking, alcohol, or drug abuse
- Lifestyle choices
- Language barriers
- Developmental barriers
- Impaired senses (hearing, vision)
- Complex therapeutic regimens
- Psychological illnesses or emotional grief
- Lack of assistive support or supervision
Environmental factors:
- Unsafe weather-related conditions
- Cluttered environments
- Insufficient automobile restraints
- Insufficient lighting
- Lack of resources or equipment
- Occupational hazards
Laboratory testing and imaging can evaluate the impact of injuries such as fractures or internal bleeding. Safety may also be preserved by avoiding injuries, such as when performing a barium swallow study to assess swallowing to prevent aspiration.
Nursing Process
Patient safety is a priority after ensuring airway stabilization and circulation. Patients receiving inpatient care are at an increased risk for injuries due to immunocompromised states, unfamiliar settings, invasive equipment and procedures, high-risk medications, and alterations in mental status. Care planning often includes elements of safety to prevent injuries and harm while inpatient and after discharge.
Nursing Assessment
Nursing professionals play a pivotal role in maintaining and enhancing patient safety through diligent assessment and intervention. This document explores the key aspects of nursing assessment and intervention in patient safety, emphasizing the importance of proactive measures to ensure optimal patient outcomes.
Initial Evaluation
The initial evaluation of a patient is critical in identifying potential safety risks and establishing a baseline for ongoing care. Key components of the initial assessment include:
Medical History: A comprehensive review of the patient’s medical history helps identify risk factors for adverse events, such as allergies, previous hospitalizations, chronic conditions, and current medications. Understanding the patient’s health background enables nurses to anticipate potential complications and tailor interventions accordingly.
Physical Examination: Conducting a thorough physical examination allows nurses to detect any signs of distress, abnormalities, or conditions that may compromise patient safety. This includes assessing vital signs, skin integrity, mobility, and cognitive function. Early detection of issues such as pressure ulcers, falls, and infections can prevent further harm.
Environmental Assessment: Evaluating the patient’s environment is essential to identify potential hazards, such as clutter, poor lighting, and unsafe equipment. Ensuring a safe and conducive environment minimizes the risk of accidents and promotes patient well-being.
Ongoing Monitoring
Continuous monitoring is vital in maintaining patient safety throughout the duration of care. Nurses must remain vigilant in recognizing and addressing emerging risks:
Vital Signs Monitoring: Regular monitoring of vital signs, including blood pressure, heart rate, respiratory rate, and temperature, helps detect early signs of deterioration. Prompt intervention can prevent complications and improve patient outcomes.
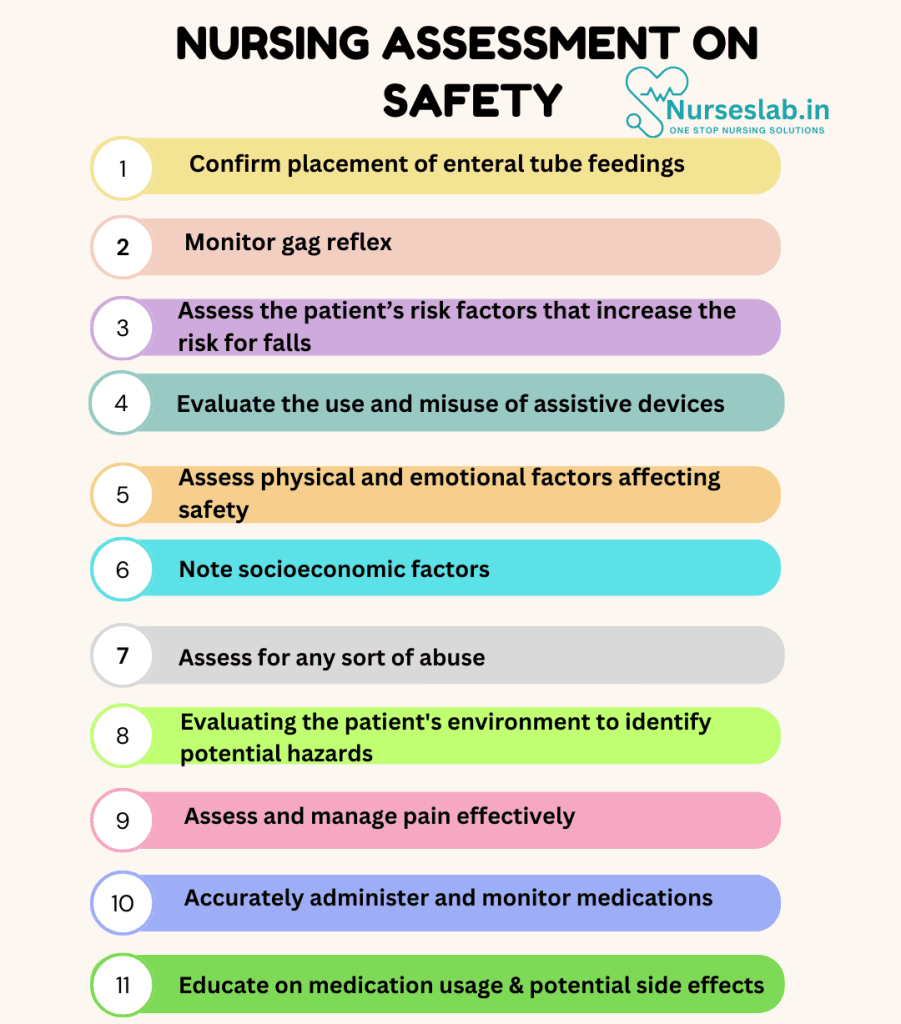
Pain Assessment: Assessing and managing pain effectively is crucial to patient safety. Uncontrolled pain can lead to physical and psychological distress, impaired mobility, and increased risk of falls. Utilizing appropriate pain assessment tools and interventions ensures patient comfort and safety.
Medication Management: Accurate administration and monitoring of medications are paramount to patient safety. Nurses must verify medication orders, administer medications correctly, and monitor for adverse reactions. Patient education on medication usage and potential side effects is also essential.
Nursing Intervention
Nursing interventions are integral to maintaining and promoting patient safety. By conducting thorough assessments, implementing preventive measures, educating and empowering patients, and fostering collaborative care, nurses play a crucial role in ensuring optimal patient outcomes.
Preventive Measures
Implementing preventive measures is a key aspect of nursing intervention to enhance patient safety. This includes:
Fall Prevention: Falls are a leading cause of injury in healthcare settings. Nurses can implement strategies such as bed alarms, non-slip footwear, and frequent patient rounds to reduce the risk of falls. Educating patients on safe mobility practices and providing assistance as needed further enhances safety.
Infection Control: Adhering to strict infection control practices is vital to preventing healthcare-associated infections. This involves proper hand hygiene, use of personal protective equipment, and aseptic techniques during procedures. Regular cleaning and disinfection of the patient environment also play a critical role.
Pressure Ulcer Prevention: To prevent pressure ulcers, nurses should conduct regular skin assessments, reposition patients frequently, and use pressure-relieving devices. Ensuring adequate nutrition and hydration further supports skin integrity.
Patient Education and Empowerment
Educating and empowering patients is fundamental to promoting patient safety. Nurses should:
Provide Comprehensive Education: Educate patients and their families about their condition, treatment plan, and potential risks. Clear and concise communication ensures patients are well-informed and can participate actively in their care.
Encourage Patient Participation: Involving patients in decision-making and care planning fosters a sense of ownership and responsibility. Encourage patients to ask questions, voice concerns, and report any changes in their condition.
Promote Health Literacy: Assess and address any barriers to understanding health information. Use plain language, visual aids, and teach-back methods to ensure patients comprehend and can apply the information provided.
Collaborative Care
Collaboration among healthcare professionals is essential to ensuring patient safety. Nurses should:
Communicate Effectively: Maintain open and effective communication with the healthcare team. Use standardized communication tools, such as SBAR (Situation-Background-Assessment-Recommendation), to convey critical information accurately.
Coordinate Care: Work collaboratively with other healthcare professionals to develop and implement a comprehensive care plan. This includes coordinating transitions of care, such as hospital discharge and follow-up appointments, to ensure continuity and safety.
Report and Address Safety Concerns: Encourage a culture of safety by reporting any safety concerns, near-misses, or adverse events promptly. Participate in root cause analysis and quality improvement initiatives to prevent recurrence and enhance patient safety practices.
Nursing Care Plans
Once the nurse identifies nursing diagnoses related to patient safety, nursing care plans help prioritize assessments and interventions for both short and long-term goals of care. In the following section, you will find nursing care plan examples related to patient safety.
Risk for Aspiration
Some patients may be at risk of inhaling substances into the tracheobronchial passages.
Nursing Diagnosis: Risk for Aspiration
Related to:
- Reduced level of consciousness
- Depressed cough/gag reflexes
- Impaired swallowing
- Impaired protective reflexes
- Oral/facial surgery or trauma
- Stroke/paralysis
- Presence of tracheostomy
- Tube feedings
As evidenced by:
A risk diagnosis is not evidenced by signs and symptoms as the problem has not yet occurred, and the goal of nursing interventions is aimed at prevention.
Expected outcomes:
- Patient will maintain a clear airway.
- Patient will not experience aspiration episodes as evidenced by the following indicators:
- Absence of coughing after swallowing
- Absence of hoarseness
- No pocketing of food
- No changes in respiratory status or lung sounds
- No alterations in LOC
Assessment:
1. Confirm placement of enteral tube feedings.
Tube placement may be evaluated through an x-ray, pH test, or auscultation at the bedside. Patients who are intubated, with a decreased level of consciousness or neurological impairment, are at increased risk of aspiration.
2. Monitor gag reflex.
The gag/swallow reflex can be assessed at the bedside before offering food or liquids. Any concerns should be further assessed through a swallow study.
Interventions:
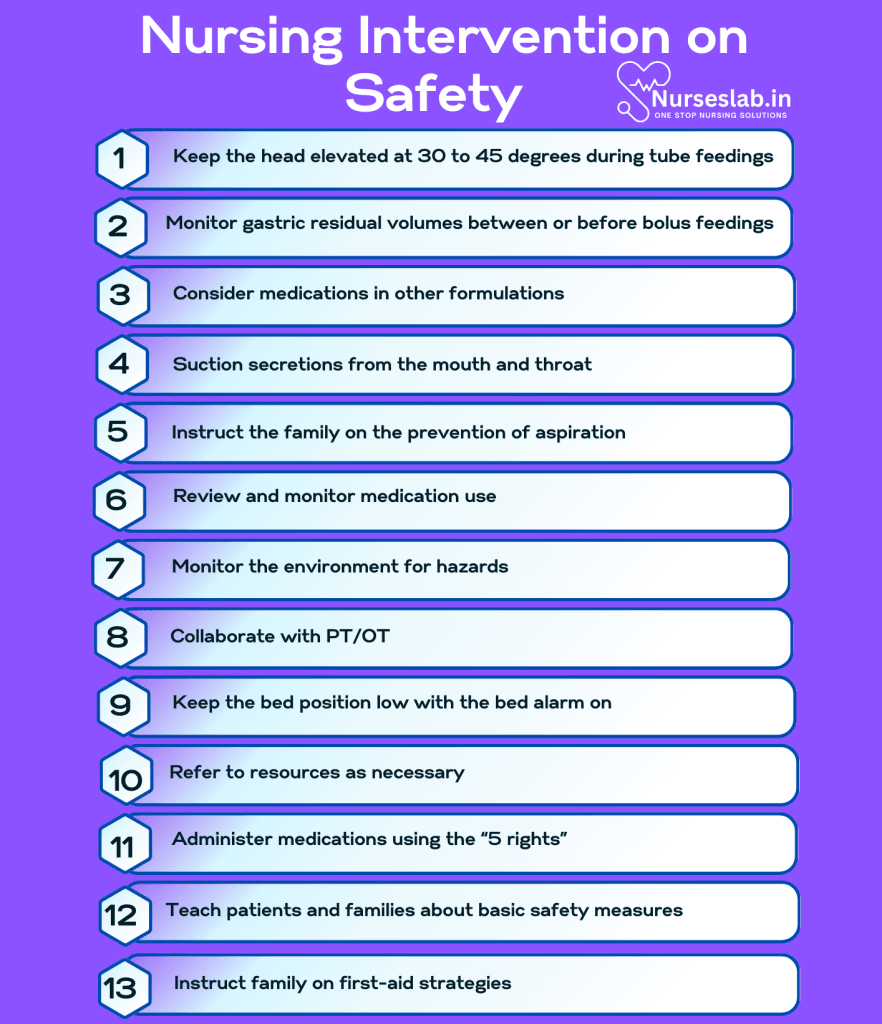
1. Keep the head elevated at 30 to 45 degrees during tube feedings.
Head elevation helps to prevent reflux due to reverse gravity. The head of the bed should be maintained at this level for an hour after feedings.
2. Monitor gastric residual volumes between or before bolus feedings.
Large gastric residuals may suggest poor digestion or an incompetent esophageal sphincter that results in aspiration. Hold feedings and contact the physician for further instructions.
3. Consider medications in other formulations.
Patients with difficulty swallowing pills, especially children, may need medications crushed or prescribed as a liquid or disintegrating tablet.
4. Suction secretions from the mouth and throat.
Suctioning secretions aids in clearing the airway. Tracheostomies often require frequent suctioning to remove mucus.
5. Instruct the family on the prevention of aspiration.
Patients who need to be fed should be monitored during mealtimes. Do not rush feedings, provide small bites, encourage chewing, and consider foods that are easier to swallow.
Risk for Falls
Patients may be at risk for falls for any number of reasons.
Nursing Diagnosis: Risk for Falls
Related to:
- Altered glucose levels
- Decreased lower extremity strength and balance
- Unsafe, cluttered environment
- Use of assistive devices
- Acute illnesses
- Chronic conditions that affect mobility
- Older age
- Environmental hazards
- Disorientation
As evidenced by:
A risk diagnosis is not evidenced by signs and symptoms as the problem has not yet occurred, and the goal of nursing interventions is aimed at prevention.
Expected outcomes:
- Patient will not experience any falls.
- Patient will demonstrate measures to prevent falls.
Assessment:
1. Assess the patient’s risk factors that increase the risk for falls.
Patients aged >65 or <2 years old, or those with chronic debilitating diseases, polypharmacy, recent trauma, on prolonged bed rest, etc., are at increased risk for falls. Fall-risk scales may be used to assess patient risk accurately.
2. Evaluate the use and misuse of assistive devices.
Assess the patient’s gait and the need for equipment. If using equipment, observe that the patient is using it correctly.
Interventions:
1. Review and monitor medication use.
Medications such as sedatives and narcotics increase drowsiness and falls if the patient is not used to their effects. Continuously monitor the effects of a new medication that could cause confusion or impairment and educate the patient on these side effects prior to discharge.
2. Monitor the environment for hazards.
Unfamiliarity increases the risk of falls. Patients receiving IV fluids may get tangled in their IV lines or trip over their pump. Other equipment in the room, such as oxygen tubing or sequential compression devices, can present a falling hazard.
3. Collaborate with PT/OT.
Patients may need instruction on exercises to increase strength, coordination, or balance. Physical/occupational therapists can recommend equipment that can benefit the patient in keeping them safe.
4. Keep the bed position low with the bed alarm on.
Patients who are identified as a high risk for falls should always have their bed kept in a low position with the bed alarm on anytime staff is not at the bedside.
Risk for Injury
The patient is vulnerable to injury from internal and external causes.
Nursing Diagnosis: Risk for Injury
Related to:
- Altered cerebral function
- Impaired mobility
- Loss of limbs
- Impaired vision
- Hearing impairment
- Malnutrition
- Psychosis
- Medication side effects
- Chemicals
- Immunosuppression
As evidenced by:
A risk diagnosis is not evidenced by signs and symptoms as the problem has not yet occurred, and the goal of nursing interventions is aimed at prevention.
Expected outcomes:
- Patient will identify factors that increase the risk of injury.
- Patient will utilize safety measures to prevent injury.
- Patient will remain free of injury.
Assessment:
1. Assess physical and emotional factors affecting safety.
Patients may be at an increased risk for injury due to disturbed thought processes, grief, lack of sleep, recent trauma, major health changes, and more that can affect their decision-making abilities.
2. Note socioeconomic factors.
A lack of housing, transportation, or access to resources increases the potential of injuries from improper self-care and medical support.
3. Assess for abuse.
The nurse is a mandated reporter of abuse. The nurse can assess for bruises in different stages of healing, frequent fractures, or question patients about emotional or verbal abuse.
Interventions:
1. Refer to resources as necessary.
Prevent injuries by ensuring vulnerable patients are receiving competent care. Children, adults with developmental delays, and older adults with dementia may need in-home care or daycare services.
2. Administer medications using the “5 rights”.
Nurses are less likely to make mistakes when double-checking medications for the right patient, medication, dose, route, and time. If medication scanners are available, they should be used and not bypassed.
3. Teach patients and families about basic safety measures.
Injury prevention requires the family’s awareness and adherence (i.e., only using medical equipment as advised, wearing seatbelts, and keeping cleaning products and medications locked away).
4. Instruct family on first-aid strategies.
Even with prevention, accidents and injuries occur. Teaching families about first aid strategies facilitates swift interventions and prevents further complications.
Nursing Diagnoses and Rationales for Patient Safety
1. Risk for Confusion
Rationale: Elevated calcium levels can affect cognitive function, leading to confusion and altered mental status. Regularly assessing neurological status and providing a safe environment can help manage confusion.
2. Risk for Imbalanced Nutrition: Less than Body Requirements
Rationale: Hypercalcemia can cause anorexia and nausea, leading to reduced food intake. Monitoring nutritional status, providing small, frequent meals, and considering nutritional supplements can help ensure adequate nutrition.
3. Deficient Knowledge
Rationale: Patients may not fully understand the implications of hypercalcemia. Educating patients and their families about the condition, its causes, symptoms, and management strategies can help them better manage their health.
4. Risk for Impaired Skin Integrity
Rationale: Dehydration and immobility associated with hypercalcemia can increase the risk of pressure ulcers. Regular skin assessments, encouraging mobility, and providing appropriate skin care can help maintain skin integrity.
5. Risk for Complications
Rationale: Chronic hypercalcemia can lead to serious complications such as kidney damage, bone pain, and cardiovascular issues. Educating patients about the importance of regular follow-up appointments, adherence to prescribed treatments, and lifestyle modifications can help prevent and manage these complications.
REFERENCES
- Appeadu MK, Bordoni B. Falls and Fall Prevention In The Elderly. [Updated 2022 Feb 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK560761/
- Bazakis AM, Kong EL, Deibel JP. Fatal Accidents. [Updated 2022 Sep 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK482328/
- Carpenito, L.J. (2013). Nursing diagnosis: Application to clinical practice. (14th ed.). Lippincott Williams & Wilkins.
- Doenges, M. E., Moorhouse, M.F., & Murr, A.C. (2019). Nursing care plans: Guidelines for individualizing client care across the life span. (10th ed.). F.A. Davis.
- American Nurses Association. (2024). Nursing: Scope and Standards of Practice (4th ed.). American Nurses Association.
- Butcher, H. K., Bulechek, G. M., Dochterman, J. M., & Wagner, C. M. (2023). Nursing Interventions Classification (NIC) (8th ed.). Elsevier.
- Herdman, T. H., & Kamitsuru, S. (2024). NANDA International Nursing Diagnoses: Definitions and Classification 2024-2026. Thieme.
- Joint Commission. (2024). National Patient Safety Goals Effective January 2024. The Joint Commission Journal on Quality and Patient Safety.
- Potter, P. A., Perry, A. G., Stockert, P. A., & Hall, A. M. (2023). Fundamentals of Nursing (10th ed.). Elsevier.
- World Health Organization. (2024). Global Patient Safety Action Plan 2024-2030. WHO Press.
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.




