


Last Updated on May 28, 2026 by Nurseslab.in Editorial Team
The study of anatomy forms the foundation of nursing practice. Understanding the structure and function of the oesophagus is vital for nurses, as disorders of this organ are common and often require skilled nursing care.
Introduction
The oesophagus, or food pipe, is a crucial component of the digestive system. For nurses, a thorough understanding of its anatomy and physiology is essential to recognise, assess, and manage patients with related disorders. This is to provide a detailed explanation exceeding 1800 words, focusing on the practical aspects relevant to nursing care. You will find information on the structure, function, and clinical significance of the oesophagus, supported by explanations suited for both students and practicing nurses.
Overview of the Oesophagus
Definition and General Function
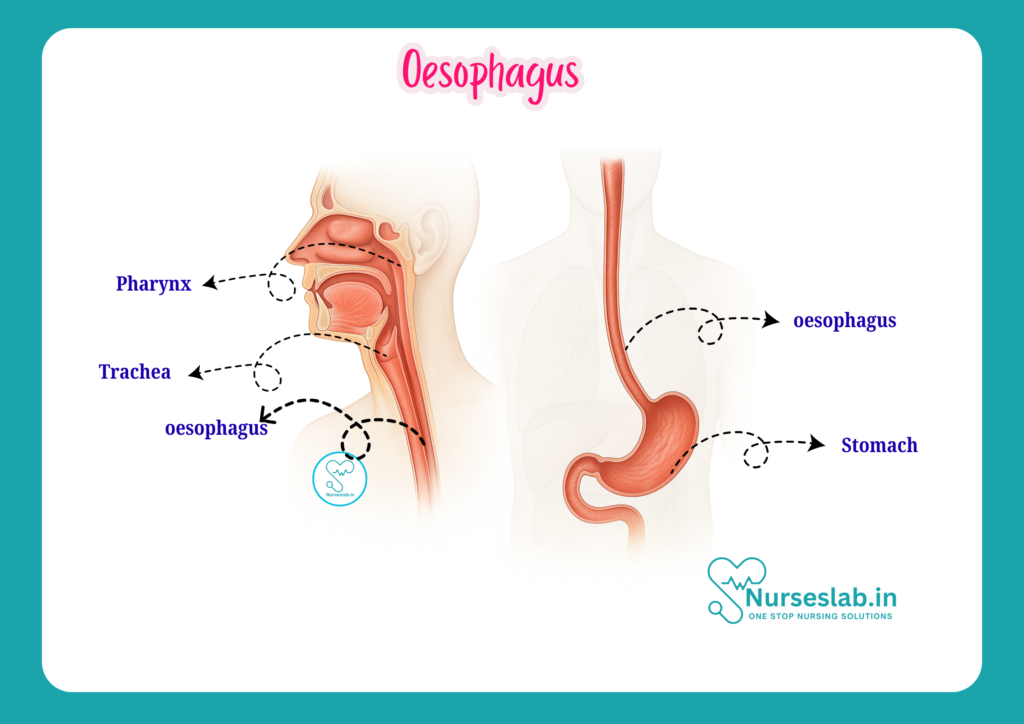
The oesophagus is a muscular tube that connects the pharynx (throat) to the stomach. Its primary function is to transport food and liquids from the mouth to the stomach for digestion. This process involves coordinated muscular contractions known as peristalsis. The oesophagus also plays a role in preventing the backflow of stomach contents, thanks to specialised sphincters at both ends.
Significance in the Digestive System
As the first segment of the gastrointestinal tract after the pharynx, the oesophagus is essential for the safe passage of ingested material. Any disruption in its function can lead to serious clinical consequences, including aspiration, malnutrition, and discomfort.
Anatomical Structure
Length, Shape, and Divisions
The adult oesophagus measures approximately 25 cm in length, though this can vary slightly based on individual anatomy. It is a straight, collapsible tube with a slight curvature to the left as it descends through the thorax. The oesophagus is conventionally divided into three parts:
- Cervical Part: This segment lies in the neck, extending from the lower border of the cricoid cartilage (at the level of the sixth cervical vertebra) to the thoracic inlet.
- Thoracic Part: The longest segment, it extends from the thoracic inlet to the diaphragm, passing through the posterior mediastinum.
- Abdominal Part: The shortest segment, approximately 1–2 cm, lies below the diaphragm and connects to the cardiac orifice of the stomach.
Anatomical Relations
Understanding the relations of the oesophagus is important for clinical practice, especially during procedures and in the assessment of trauma or disease.
- Anteriorly: The trachea and left atrium of the heart lie in front of the oesophagus in the neck and upper thorax, respectively.
- Posteriorly: The vertebral column and descending thoracic aorta are located behind the oesophagus.
- Lateral Relations: The carotid sheaths (containing the carotid arteries and jugular veins) are lateral in the neck; the lungs and pleura are lateral in the thorax.
The oesophagus passes through the oesophageal hiatus of the diaphragm at the level of the tenth thoracic vertebra (T10).
Histology
Layers of the Oesophagus
The wall of the oesophagus consists of four main layers, each with distinct structural and functional properties:
- Mucosa: The innermost layer, lined by non-keratinised stratified squamous epithelium, designed to protect against abrasion from food. Beneath the epithelium lies the lamina propria (connective tissue) and muscularis mucosae (thin muscle layer).
- Submucosa: Contains dense connective tissue, blood vessels, lymphatics, and submucosal glands that secrete mucus to lubricate the lumen.
- Muscularis Externa: Composed of two layers of muscle – an inner circular and an outer longitudinal layer. The upper third consists of skeletal muscle, the middle third is a mix of skeletal and smooth muscle, and the lower third is entirely smooth muscle. This arrangement is crucial for the initiation and propagation of peristalsis.
- Adventitia/Serosa: The outermost layer is primarily adventitia (loose connective tissue) in the neck and thorax, which blends with surrounding structures. In the abdominal part, the oesophagus is covered by a serosa (visceral peritoneum).
Cell Types and Functional Significance
The stratified squamous epithelium is resistant to mechanical stress, while mucus-secreting glands in the submucosa facilitate smooth passage of food. The muscular arrangement allows voluntary initiation of swallowing, followed by involuntary peristaltic movement, ensuring efficient transit to the stomach.
Blood Supply
Arterial Supply
The blood supply of the oesophagus is segmental and varies along its length:
- Cervical Part: Supplied by branches of the inferior thyroid artery.
- Thoracic Part: Receives blood from oesophageal branches of the thoracic aorta and bronchial arteries.
- Abdominal Part: Supplied by branches of the left gastric artery (from the coeliac trunk) and the left inferior phrenic artery.
Venous Drainage
Venous drainage also varies:
- Cervical Oesophagus: Drains into the inferior thyroid veins.
- Thoracic Oesophagus: Drains into the azygos and hemiazygos veins.
- Abdominal Oesophagus: Drains into the left gastric vein, which is a tributary of the portal vein.
This anatomical arrangement is clinically important because the lower oesophageal veins form a portosystemic anastomosis. In portal hypertension, these veins can become dilated, leading to oesophageal varices—a life-threatening condition due to the risk of bleeding.
Nerve Supply
Parasympathetic and Sympathetic Innervation
The oesophagus receives a rich nerve supply that coordinates its motor and sensory functions:
- Parasympathetic Supply: Vagus nerve (cranial nerve X) provides motor fibres to the muscle, facilitating peristalsis and relaxation of the sphincters.
- Sympathetic Supply: Sympathetic fibres arise from the cervical and thoracic sympathetic trunks (T1–T6), primarily regulating blood flow and modulating muscle tone.
Enteric Nervous System
Within the oesophageal wall, the enteric nervous system (ENS)—comprising the myenteric (Auerbach’s) and submucosal (Meissner’s) plexuses—controls local reflexes, peristalsis, and glandular secretion.
Role in Peristalsis
Peristalsis is the coordinated contraction and relaxation of oesophageal muscles, propelling food towards the stomach. The ENS integrates signals from both central and local sources to ensure smooth, timely movement. Disorders affecting nerve supply can lead to motility problems such as achalasia.
Lymphatic Drainage
Lymph Node Groups
Lymphatic drainage of the oesophagus is complex and clinically significant, especially for the spread of malignancy:
- Cervical Oesophagus: Drains into deep cervical and paratracheal lymph nodes.
- Thoracic Oesophagus: Drains into posterior mediastinal and tracheobronchial lymph nodes.
- Abdominal Oesophagus: Drains into left gastric and coeliac lymph nodes.
Clinical Implications
Because lymphatic channels cross anatomical boundaries, cancer of the oesophagus can spread rapidly to distant lymph nodes, complicating treatment and prognosis. Nurses should be aware of the patterns of lymphatic spread when caring for patients with oesophageal cancer or infection.
Physiological Functions
Swallowing Mechanism
Swallowing (deglutition) is a complex, multi-phase process:
- Oral Phase: Voluntary; food is chewed and formed into a bolus, which is pushed to the back of the mouth.
- Pharyngeal Phase: Involuntary; the bolus passes through the pharynx into the oesophagus, while the epiglottis closes to prevent aspiration.
- Oesophageal Phase: Involuntary; peristaltic waves carry the bolus down the oesophagus to the stomach.
Peristalsis
Peristalsis involves sequential contraction of the circular and longitudinal muscle layers, coordinated by the ENS and modulated by autonomic nerves. This action is critical for the efficient movement of food and liquids.
Sphincters
- Upper Oesophageal Sphincter (UOS): Located at the junction with the pharynx, composed mainly of the cricopharyngeus muscle. It prevents air from entering the oesophagus during breathing and protects against reflux of oesophageal contents into the pharynx.
- Lower Oesophageal Sphincter (LOS): Located at the junction with the stomach, it is a physiological sphincter (not a distinct anatomical structure). It prevents reflux of gastric contents into the oesophagus, protecting the mucosa from acid injury.
Clinical Significance
Common Disorders
Several disorders of the oesophagus are commonly encountered in clinical practice. Nurses play a key role in recognising symptoms, providing care, and educating patients.
1. Gastro-Oesophageal Reflux Disease (GERD):
- GERD occurs when the lower oesophageal sphincter fails to prevent stomach acid from refluxing into the oesophagus. Symptoms include heartburn, regurgitation, and sometimes chest pain. Chronic GERD can lead to complications such as Barrett’s oesophagus and oesophageal strictures. Nurses should monitor for signs of aspiration, educate patients on lifestyle modifications (e.g., weight reduction, dietary changes), and administer prescribed medications such as antacids and proton pump inhibitors.
2. Achalasia:
- This is a motility disorder characterised by failure of the lower oesophageal sphincter to relax and loss of peristalsis in the oesophageal body. Patients present with dysphagia (difficulty swallowing), regurgitation, and sometimes chest pain. Nurses should assess swallowing ability, provide guidance on dietary modifications (soft foods, small meals), and support patients undergoing procedures such as pneumatic dilation or surgical myotomy.
- Oesophageal Strictures:
- Strictures are abnormal narrowing of the oesophagus, often due to chronic inflammation, GERD, or caustic injury. Symptoms include progressive dysphagia and risk of food impaction. Nurses should monitor nutritional status, assist with endoscopic procedures, and educate patients on preventing further injury.
3. Oesophageal Cancer:
- Malignancy may arise from squamous cells (upper and middle oesophagus) or glandular cells (lower oesophagus). Symptoms include progressive dysphagia, weight loss, and sometimes pain. Nurses must be vigilant for signs of obstruction, aspiration, and provide emotional and physical support. Understanding lymphatic drainage is critical for staging and management. Palliative care, nutritional support, and pain management are important nursing considerations.
4. Oesophageal Varices:
- These are dilated submucosal veins in the lower oesophagus, typically due to portal hypertension secondary to liver disease. Varices pose a high risk of life-threatening bleeding. Nurses should monitor for signs of haematemesis (vomiting blood), hypotension, and shock, and assist in emergency management, including administration of vasoactive drugs and blood products.
Symptoms and Nursing Considerations
Common symptoms of oesophageal disorders include dysphagia, odynophagia (painful swallowing), heartburn, regurgitation, chest pain, and weight loss. Nurses should conduct thorough assessments, monitor for complications (aspiration, malnutrition), and provide holistic care including patient education, emotional support, and coordination with multidisciplinary teams.
Summary and Key Points
- The oesophagus is a muscular tube connecting the pharynx to the stomach, essential for transporting food and liquids.
- Anatomically, it is divided into cervical, thoracic, and abdominal parts, each with specific relations and clinical relevance.
- Its wall consists of four layers: mucosa, submucosa, muscularis externa, and adventitia/serosa, each serving a protective and functional role.
- Blood supply is segmental; venous drainage is significant for the development of varices in portal hypertension.
- Nerve supply involves both autonomic and enteric components, coordinating peristalsis and sphincter function.
- Lymphatic drainage is crucial in the spread of infection and malignancy.
- The main physiological functions are swallowing, peristalsis, and prevention of reflux via sphincters.
- Common disorders include GERD, achalasia, strictures, cancer, and varices; nursing care focuses on assessment, management, and patient education.
A sound understanding of oesophageal anatomy and function enables nurses to provide effective care, anticipate complications, and contribute meaningfully to patient outcomes.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.



