


Last Updated on May 27, 2026 by Nurseslab.in Editorial Team
Introduction
Understanding the anatomy of the large intestine is crucial for nurses, as it plays a vital role in maintaining digestive health and overall well-being. The large intestine is responsible for the absorption of water and electrolytes, the formation and expulsion of faeces, and houses a complex microbial ecosystem.
Overview of the Large Intestine
The large intestine, also known as the large bowel, is the terminal part of the digestive tract, extending from the ileocaecal junction to the anus. It is approximately 1.5 metres (about 5 feet) in length and 6-7 cm in diameter, making it wider but shorter than the small intestine.
Located in the abdominal and pelvic cavities, the large intestine frames the coiled loops of the small intestine. Its primary role is to absorb water and electrolytes from indigestible food residues, convert them into solid waste (faeces), and facilitate their elimination from the body. The large intestine also provides a habitat for beneficial gut flora, which play a significant role in maintaining health.
Anatomical Divisions of the Large Intestine
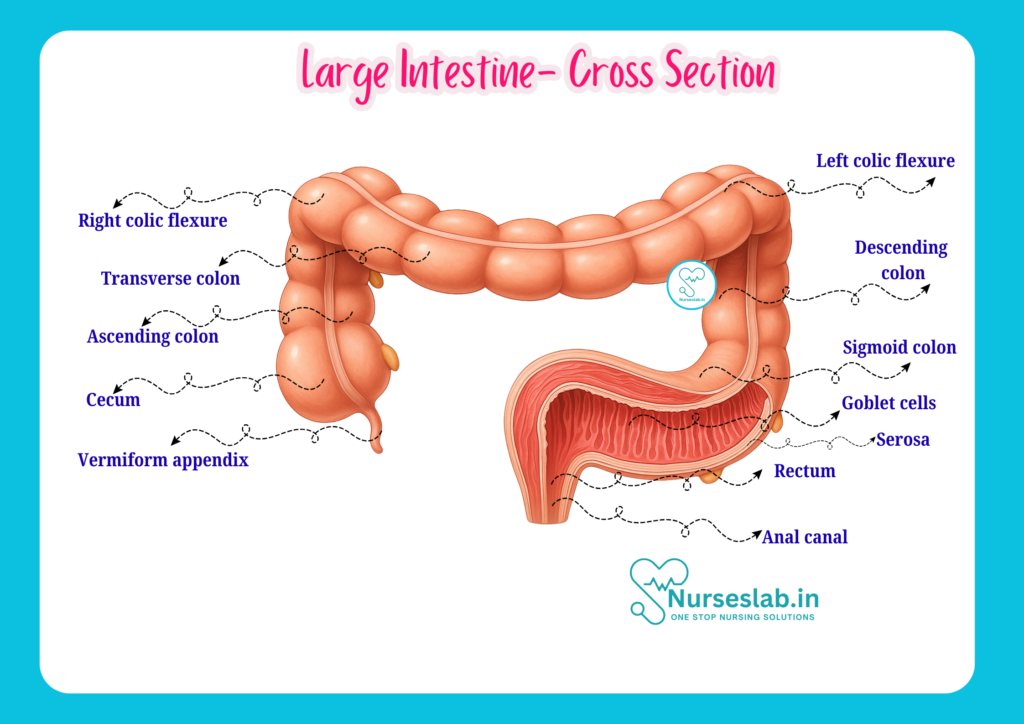
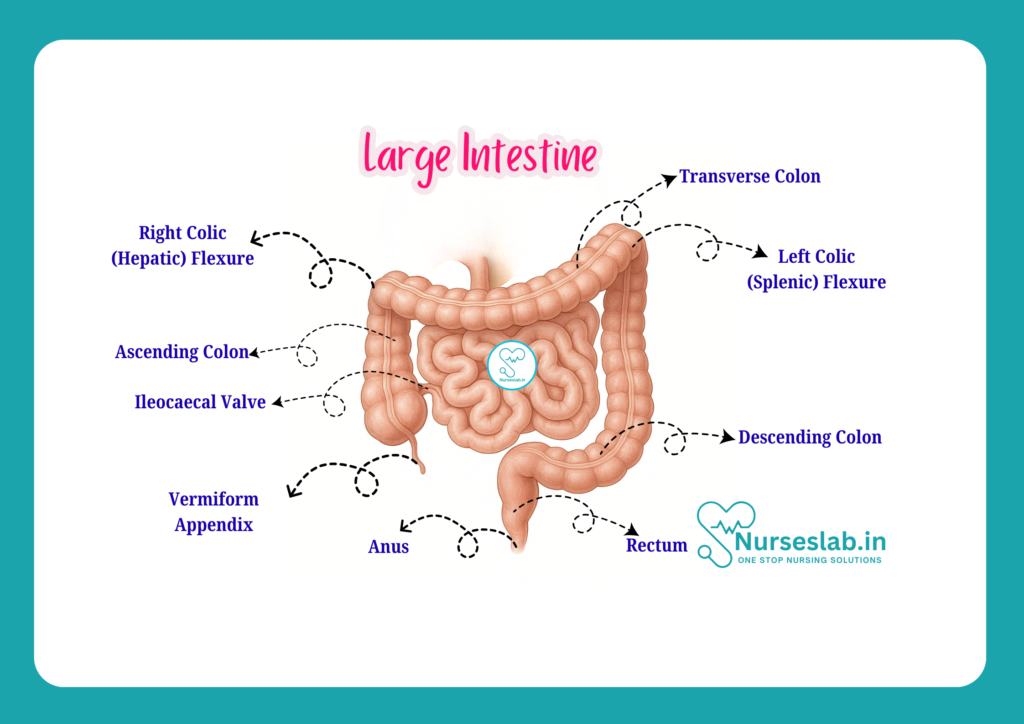
The large intestine is divided into several distinct anatomical regions, each with unique structural and functional characteristics. These regions include the caecum, appendix, colon (further subdivided into ascending, transverse, descending, and sigmoid sections), rectum, and anal canal.
Caecum
The caecum is a pouch-like structure situated in the right lower quadrant of the abdomen, just below the ileocaecal valve where the small intestine ends. Measuring about 6 cm in length and width, it acts as a receiving chamber for chyme (partially digested food) from the ileum. The caecum plays a role in absorbing fluids and salts that remain after intestinal digestion and absorption.
Appendix
Attached to the posteromedial wall of the caecum is the vermiform appendix, a narrow, worm-shaped tube measuring about 7-10 cm in length. The appendix contains lymphoid tissue and is thought to have an immunological function, especially in early life. Its location is variable, but it is most commonly found in a retrocaecal position. Acute inflammation of the appendix, known as appendicitis, is a common clinical problem.
Colon
The colon is the longest part of the large intestine and is subdivided into four regions:
- Ascending Colon: Extends upward from the caecum along the right side of the abdominal cavity to the level of the liver, ending at the hepatic flexure.
- Transverse Colon: Crosses the abdomen from right to left, passing below the stomach and in front of the pancreas. It ends at the splenic flexure near the spleen.
- Descending Colon: Travels downward on the left side of the abdomen from the splenic flexure to the iliac fossa.
- Sigmoid Colon: An S-shaped segment that connects the descending colon to the rectum. It is located in the pelvis and is highly mobile.
The colon is characterised by sacculations known as haustra, longitudinal bands of muscle termed taeniae coli, and fatty appendages called appendices epiploicae.
Rectum
The rectum is the final straight portion of the large intestine, measuring approximately 12-15 cm in length. It lies in the pelvic cavity and serves as a temporary storage site for faeces before defaecation. The rectum follows the curve of the sacrum and ends at the anorectal junction.
Anal Canal
The anal canal is the terminal segment of the large intestine, about 3-4 cm long, passing through the pelvic floor muscles. It is surrounded by internal and external anal sphincters that control the passage of faeces. The canal is lined by specialised mucosa and is highly sensitive, which is important for the maintenance of continence.
Histology and Structural Layers
The wall of the large intestine is composed of four principal layers, each with distinct structural and functional roles:
- Mucosa: The innermost layer, lined by simple columnar epithelium interspersed with goblet cells, which secrete mucus to lubricate the passage of faeces. The mucosa contains numerous tubular glands called crypts of Lieberkühn but lacks villi, differentiating it from the small intestine.
- Submucosa: This layer consists of loose connective tissue containing blood vessels, lymphatics, and nerves. It supports the mucosa and provides the necessary vascular and neural connections.
- Muscularis Externa: Composed of an inner circular and an outer longitudinal muscle layer. The longitudinal layer is gathered into three thick bands (taeniae coli) that run the length of the colon, creating the haustral pattern. In the rectum and anal canal, the muscular layers become more uniform and robust, facilitating the expulsion of faeces.
- Serosa (or Adventitia): The outermost covering of the intraperitoneal parts is the serosa, a smooth membrane that secretes serous fluid to reduce friction. The retroperitoneal parts are covered by adventitia, a connective tissue layer.
Blood Supply and Lymphatic Drainage
Arterial Supply
The large intestine receives its blood supply from branches of the superior mesenteric artery (SMA) and inferior mesenteric artery (IMA).
- Superior Mesenteric Artery: Supplies the caecum, appendix, ascending colon, and the proximal two-thirds of the transverse colon via the ileocolic, right colic, and middle colic arteries.
- Inferior Mesenteric Artery: Supplies the distal one-third of the transverse colon, descending colon, sigmoid colon, and the upper part of the rectum via the left colic, sigmoid, and superior rectal arteries.
- Other Arteries: The lower part of the rectum and anal canal receive blood from the middle and inferior rectal arteries, branches of the internal iliac artery.
Venous Drainage
Venous blood from the large intestine generally parallels the arterial supply. The veins ultimately drain into the portal venous system:
- Superior mesenteric vein: Drains the caecum, appendix, ascending colon, and most of the transverse colon.
- Inferior mesenteric vein: Drains the descending and sigmoid colon, as well as the upper rectum; it typically joins the splenic vein before forming the portal vein.
- Rectal venous plexus: The lower rectum and anal canal drain into the systemic venous system via the internal iliac veins. This dual drainage creates portosystemic anastomoses, clinically significant in conditions like portal hypertension.
Lymphatic Drainage
Lymph from the large intestine drains into a series of nodes that follow the blood vessels:
- Epicolic and paracolic nodes (on and near the intestine)
- Intermediate nodes (along the main vessels)
- Principal nodes (near the origins of the main arteries)
The lymph ultimately drains into the superior and inferior mesenteric lymph nodes, and then to the cisterna chyli, which leads to the thoracic duct.
Nerve Supply
The large intestine receives both sympathetic and parasympathetic innervation, which regulate its motility, secretion, and blood flow.
- Sympathetic Innervation: Provided by the thoracic and lumbar splanchnic nerves, with fibres synapsing in the superior and inferior mesenteric ganglia. Sympathetic stimulation inhibits peristalsis and secretion, and constricts blood vessels.
- Parasympathetic Innervation: The vagus nerve supplies parasympathetic fibres to the caecum, appendix, ascending colon, and proximal transverse colon, enhancing motility and secretion. The distal transverse colon, descending colon, sigmoid colon, rectum, and anal canal receive parasympathetic supply from the pelvic splanchnic nerves (S2-S4).
- Enteric Nervous System: The myenteric (Auerbach’s) and submucosal (Meissner’s) plexuses coordinate local reflex activities such as peristalsis and secretion.
Physiological Functions
The large intestine performs several essential physiological functions:
- Absorption: The large intestine absorbs water (up to 1.5 litres per day) and electrolytes (particularly sodium and chloride ions) from the luminal contents, transforming liquid chyme into semi-solid faeces.
- Formation and Expulsion of Faeces: Indigestible residues are compacted into faeces, which are temporarily stored in the rectum before being expelled through the anus during defaecation. The process is regulated by complex neural and muscular mechanisms.
- Gut Flora (Microbiota): The colon hosts trillions of beneficial bacteria that aid in the fermentation of undigested carbohydrates, synthesis of certain vitamins (e.g., vitamin K, some B-vitamins), and protection against pathogenic microbes. These bacteria also contribute to the production of short-chain fatty acids, which are important for colonic health.
- Water and Electrolyte Balance: By absorbing water and salts, the large intestine helps maintain the body’s fluid and electrolyte homeostasis.
Clinical Significance
A detailed understanding of the large intestine’s anatomy is essential for recognising, preventing, and managing a variety of clinical conditions. Some of the most common and significant disorders include:
Colorectal Cancer
Colorectal cancer is a leading cause of cancer-related morbidity and mortality. It often arises from adenomatous polyps and is more common in older adults. Early detection through screening (such as colonoscopy) and awareness of symptoms (e.g., altered bowel habits, bleeding per rectum) are crucial for effective management. Nurses play a vital role in patient education, screening, and care during treatment.
Appendicitis
Acute inflammation of the appendix, known as appendicitis, is a common surgical emergency. Classic symptoms include right lower abdominal pain, fever, and vomiting. Delay in diagnosis can lead to perforation, peritonitis, and sepsis. Nurses are often the first to assess patients and must be vigilant for signs of acute abdomen.
Diverticulosis and Diverticulitis
Diverticulosis refers to the presence of small pouches (diverticula) in the wall of the colon, most commonly the sigmoid colon. When these pouches become inflamed or infected, the condition is termed diverticulitis, which may present with abdominal pain, fever, and altered bowel habits. Complications can include perforation and abscess formation. Dietary advice and patient monitoring are important nursing responsibilities.
Inflammatory Bowel Disease (IBD)
IBD encompasses two main disorders: ulcerative colitis and Crohn’s disease. Both are chronic inflammatory conditions affecting the colon and/or rectum, leading to symptoms such as diarrhoea, abdominal pain, rectal bleeding, and weight loss. Management may include medication, nutritional support, and sometimes surgery. Nurses provide ongoing care, education, and psychological support for patients with IBD.
Nursing Considerations
- Assessment: Careful history taking and physical examination of patients with abdominal symptoms, monitoring for signs of dehydration, electrolyte imbalance, and signs of acute abdomen.
- Patient Education: Educating patients and their families about healthy dietary habits, importance of screening and early detection of colorectal diseases, and recognising warning signs that necessitate medical attention.
- Procedural Care: Preparing patients for diagnostic procedures such as colonoscopy, barium enema, and surgery; providing post-operative care and monitoring for complications.
- Supportive Care: Addressing psychosocial aspects, managing symptoms, and coordinating care with multidisciplinary teams.
Summary and Key Points
- The large intestine is the final section of the gastrointestinal tract, responsible for water and electrolyte absorption, faecal formation, and hosting gut flora.
- It is divided into caecum, appendix, colon (ascending, transverse, descending, sigmoid), rectum, and anal canal.
- Structural layers include mucosa, submucosa, muscularis externa, and serosa/adventitia.
- Blood supply is via the superior and inferior mesenteric arteries; venous return is primarily to the portal system.
- Lymphatic drainage follows vascular supply and is clinically significant in cancer spread.
- Nerve supply includes both sympathetic and parasympathetic components.
- The large intestine’s functions include absorption, formation and expulsion of faeces, and maintaining gut health through microbiota.
- Common clinical conditions include colorectal cancer, appendicitis, diverticulosis/diverticulitis, and IBD, all of which require nursing awareness and intervention.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.




