


The nose and nasal cavity are integral components of the human respiratory system, playing vital roles beyond mere breathing.
Introduction:
Nurses are often the first healthcare professionals to assess patients presenting with respiratory complaints, facial trauma, or symptoms affecting the nose and upper airway. Knowledge of nasal anatomy underpins effective patient assessment, informs appropriate interventions, and aids in the recognition of potentially serious conditions. Moreover, understanding the nose’s roles in respiration, filtration, olfaction, and even speech resonance enhances the holistic care nurses provide.
Overview of the Nose
External Nose
The external nose is the visible part of the nose projecting from the face. It serves as the entrance to the nasal cavity and is central to facial aesthetics and function. The shape and size of the nose vary among individuals and populations, influenced by genetic and environmental factors. The external nose consists of a bony upper part and a cartilaginous lower part, both covered by skin and subcutaneous tissue.
Surface Anatomy and Landmarks
Key surface landmarks of the external nose include:
- Root: The uppermost part, located between the eyes, where the nose meets the forehead.
- Dorsum: The length of the nose, extending from the root to the tip (apex).
- Apex: The tip of the nose, often rounded and prominent.
- Alae: The lateral, flared portions on either side of the nostrils (nares).
- Nostrils (Nares): The two external openings leading into the nasal cavity.
- Columella: The soft tissue and cartilage separating the two nostrils at the base.
These landmarks are crucial for clinical assessment, especially in trauma or reconstructive procedures.
Structural Anatomy
Bones
The bony framework of the nose provides support and defines its upper third. The main bones involved are:
- Nasal Bones: Two small, oblong bones form the bridge of the nose.
- Frontal Process of the Maxilla: Contributes to the lateral aspect of the nose.
- Nasal Part of the Frontal Bone: Forms the root and upper part of the dorsum.
- Perpendicular Plate of the Ethmoid: Forms part of the nasal septum, contributing to the internal structure.
The bony vault is important for structural integrity and is often involved in nasal fractures.
Cartilage
The lower two-thirds of the nose are supported by cartilage, providing flexibility and maintaining the shape of the nostrils. Major cartilages include:
- Upper Lateral Cartilages: Paired structures that connect to the nasal bones and form the middle third of the nose.
- Lower Lateral (Alar) Cartilages: Form the tip (apex) and alae of the nose, giving shape to the nostrils.
- Septal Cartilage: A flat, quadrangular plate forming the anterior portion of the nasal septum.
- Minor Alar Cartilages and Accessory Cartilages: Small cartilaginous pieces that provide additional support.
Cartilaginous structures are susceptible to trauma and deformities, which can impact nasal function.
Muscles
Several small muscles around the nose, known as the nasal muscles, control the movement of the nostrils and contribute to facial expressions. They include:
- Nasalis: Compresses the nasal aperture and flares the nostrils.
- Procerus: Draws down the medial angle of the eyebrows, producing horizontal wrinkles over the bridge of the nose.
- Depressor Septi Nasi: Pulls the nasal septum downward, affecting nostril shape.
- Levator Labii Superioris Alaeque Nasi: Elevates the upper lip and dilates the nostrils.
These muscles are innervated by branches of the facial nerve (cranial nerve VII).
Nasal Cavity
Boundaries
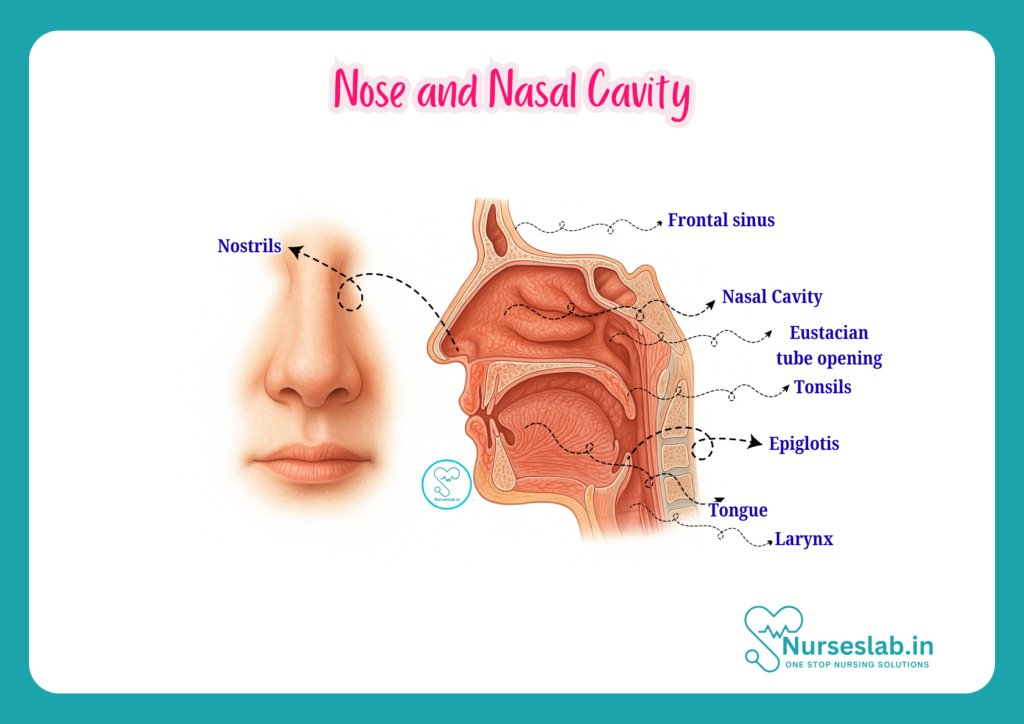
The nasal cavity is a paired, air-filled space located within the skull, extending from the nostrils (anterior nares) to the choanae (posterior nares), which open into the nasopharynx. Its boundaries are as follows:
- Roof: Formed by the nasal bones, frontal bone, cribriform plate of the ethmoid, and the body of the sphenoid.
- Floor: Composed of the palatine process of the maxilla and the horizontal plate of the palatine bone.
- Medial Wall: Primarily formed by the nasal septum.
- Lateral Wall: Irregular due to the presence of conchae (turbinates) and meatuses.
- Anterior Boundary: The nares.
- Posterior Boundary: The choanae, leading into the nasopharynx.
Divisions
Each nasal cavity can be divided into:
- Vestibule: The anterior portion, just inside the nostrils, lined by skin and vibrissae (coarse hairs) that filter large particles.
- Respiratory Region: The largest part, lined by respiratory mucosa.
- Olfactory Region: The superior part, lined by olfactory epithelium responsible for the sense of smell.
Regions
The nasal cavity is further subdivided for clinical and anatomical purposes:
- Superior Meatus: Located below the superior concha.
- Middle Meatus: Below the middle concha; most paranasal sinuses drain here.
- Inferior Meatus: Below the inferior concha; the nasolacrimal duct opens into this meatus.
Nasal Septum
Structure
The nasal septum is the partition that divides the nasal cavity into right and left halves. It has both bony and cartilaginous components:
- Cartilaginous Part: The anterior (front) portion, formed by the septal cartilage.
- Bony Part: The posterior (back) portion, formed by the perpendicular plate of the ethmoid bone and the vomer.
- Membranous Part: A small area near the nostrils, formed by connective tissue.
The septum provides structural support and directs airflow through the nasal passages.
Blood Supply
The nasal septum has a rich blood supply, primarily from branches of the:
- Anterior Ethmoidal Artery (branch of the ophthalmic artery)
- Posterior Ethmoidal Artery
- Sphenopalatine Artery (branch of the maxillary artery)
- Greater Palatine Artery
- Superior Labial Artery (branch of the facial artery)
The area known as Kiesselbach’s plexus (Little’s area) on the anterior part of the septum is a common site for nosebleeds (epistaxis).
Clinical Significance
Deviated nasal septum is a frequent finding that may cause nasal obstruction, recurrent sinusitis, or breathing difficulties. Septal perforation, trauma, and epistaxis are other important clinical considerations. Nurses should be familiar with these conditions for prompt recognition and referral.
Lateral Wall of Nasal Cavity
Conchae (Turbinates)
The lateral wall of each nasal cavity contains three curved bony projections called conchae (or turbinates):
- Superior Concha: Part of the ethmoid bone.
- Middle Concha: Also part of the ethmoid bone.
- Inferior Concha: A separate bone.
These structures increase the surface area of the nasal cavity, helping to warm, humidify, and filter the inhaled air.
Meatuses
Below each concha is a passageway called a meatus:
- Superior Meatus: Receives the opening of the posterior ethmoidal sinuses.
- Middle Meatus: Contains the semilunar hiatus where the frontal, maxillary, and anterior ethmoidal sinuses drain.
- Inferior Meatus: Receives the opening of the nasolacrimal duct (draining tears from the eyes).
Understanding the drainage pathways is crucial for recognising the spread of infection and sinusitis.
Openings
Several openings are present on the lateral wall for the drainage of paranasal sinuses and the nasolacrimal duct. These include:
- Frontal sinus opening (middle meatus)
- Maxillary sinus opening (middle meatus)
- Anterior, middle, and posterior ethmoidal sinus openings (middle and superior meatuses)
- Nasolacrimal duct opening (inferior meatus)
Blockage or infection of these openings can lead to sinusitis or dacryocystitis (inflammation of the lacrimal sac).
Mucosa and Epithelium
Types
The nasal cavity is lined by two main types of mucosa:
- Respiratory Mucosa: Pseudostratified ciliated columnar epithelium with goblet cells, covering most of the nasal cavity. It secretes mucus to trap dust and pathogens.
- Olfactory Mucosa: Specialised neuroepithelium located in the roof of the nasal cavity, containing olfactory receptor cells responsible for smell.
Functions
The mucosa performs several vital functions:
- Traps and removes particles and microorganisms from inspired air.
- Humidifies and warms the air before it passes to the lower respiratory tract.
- Contains immune cells that provide a first line of defence against pathogens.
Olfactory Region
The olfactory region is a small area on the roof of the nasal cavity and adjacent septum and superior concha. It contains olfactory receptor neurons whose axons pass through the cribriform plate to synapse in the olfactory bulb. This region is responsible for the sense of smell, which can be affected by upper respiratory infections, trauma, or neurodegenerative diseases.
Blood Supply and Innervation
Arterial Supply
The nose and nasal cavity receive a rich blood supply from both internal and external carotid artery branches. Key arteries include:
- Anterior and posterior ethmoidal arteries (from the ophthalmic artery)
- Sphenopalatine artery (from the maxillary artery)
- Greater palatine artery
- Superior labial artery (from the facial artery)
This extensive blood supply explains the frequency of nosebleeds and the rapid absorption of intranasal medications.
Venous Drainage
Venous blood from the nasal cavity drains into the facial, ophthalmic, and sphenopalatine veins. The rich venous plexus in the anterior septum (Kiesselbach’s area) is a common site for epistaxis. Some veins communicate with the cavernous sinus, providing a potential route for the spread of infection to the cranial cavity.
Nerve Supply
The sensory innervation of the nose and nasal cavity is provided by:
- Olfactory Nerve (Cranial Nerve I): Special sense of smell.
- Trigeminal Nerve (Cranial Nerve V): General sensation via its ophthalmic (V1) and maxillary (V2) divisions.
- Autonomic Nerves: Parasympathetic fibres (from the facial nerve) stimulate mucus secretion, while sympathetic fibres regulate blood flow.
Knowledge of nerve supply is important in understanding referred pain, local anaesthesia, and certain neurological conditions.
Functions of Nose and Nasal Cavity
- Respiration: The nose is the primary entry point for inspired air, which is filtered, warmed, and humidified before reaching the lungs.
- Filtration and Defence: Vibrissae, mucus, and cilia trap dust, microbes, and other particles, protecting the lower respiratory tract.
- Olfaction: The olfactory mucosa detects airborne chemicals, enabling the sense of smell, which is linked to taste and safety (e.g., detecting smoke or gas leaks).
- Resonance of Voice: The nasal cavity acts as a resonating chamber, contributing to the quality and timbre of the voice.
- Drainage: The nose facilitates drainage of tears from the eyes via the nasolacrimal duct and mucus from the paranasal sinuses.
Clinical Relevance
Common Conditions
- Rhinitis: Inflammation of the nasal mucosa, which may be allergic (hay fever) or infectious (common cold).
- Sinusitis: Infection or inflammation of the paranasal sinuses, often presenting with facial pain, congestion, and nasal discharge.
- Epistaxis: Nosebleeds, commonly arising from Kiesselbach’s plexus, may be spontaneous or traumatic.
- Deviated Nasal Septum: Displacement of the septum, leading to obstruction, snoring, or recurrent infections.
- Nasal Polyps: Benign mucosal growths causing obstruction or reduced sense of smell.
- Foreign Bodies: Especially in children, foreign objects in the nose can cause obstruction and infection.
- Trauma: Fractures of the nasal bones or septum may result from accidents or sports injuries.
- Olfactory Disorders: Loss or distortion of the sense of smell (anosmia, hyposmia) can result from infections, trauma, or neurological diseases.
Examination Techniques
Nurses play a vital role in the assessment of the nose and nasal cavity. Key techniques include:
- Inspection of the external nose for symmetry, deformity, or swelling.
- Palpation to detect tenderness, crepitus, or instability.
- Assessment of nasal airflow by occluding one nostril at a time and asking the patient to breathe.
- Visual examination of the vestibule and anterior septum using a torch and nasal speculum.
- Observation for discharge, bleeding, polyps, or foreign bodies.
- Assessment of olfactory function using familiar scents (coffee, soap).
Careful documentation and prompt referral for abnormalities are vital nursing responsibilities.
Nursing Considerations
Nursing care for patients with nasal conditions includes:
- Educating patients about nasal hygiene and the importance of avoiding nose picking or blowing too forcefully.
- Assisting with nasal irrigation or medication administration (e.g., nasal sprays, drops).
- Monitoring for complications such as severe bleeding, airway compromise, or signs of infection.
- Providing post-operative care following nasal surgery, including wound care, pain management, and infection prevention.
- Supporting patients with olfactory disorders by addressing safety concerns (e.g., inability to smell smoke or gas leaks).
Summary and Key Takeaways
The nose and nasal cavity are complex anatomical structures with essential roles in respiration, defence, olfaction, and communication. For nurses, detailed knowledge of their anatomy and functions is crucial for effective assessment, recognition of pathology, and patient education. Key points include:
- The external nose comprises bony and cartilaginous frameworks, with important surface landmarks for clinical assessment.
- The nasal cavity is divided into vestibular, respiratory, and olfactory regions, each with distinct features and functions.
- The nasal septum and lateral wall (conchae and meatuses) are central to nasal airflow, drainage, and filtration.
- Rich blood supply and innervation explain common symptoms and complications such as epistaxis and referred pain.
- Nurses must be adept at examining the nose, recognising common conditions, and providing holistic care for patients with nasal issues.
A sound understanding of nasal anatomy equips nursing professionals to contribute effectively to patient care, health promotion, and the multidisciplinary healthcare team.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.




