


Last Updated on May 27, 2026 by Nurseslab.in Editorial Team
The gall bladder is a crucial organ in the digestive system, and a sound understanding of its anatomy is essential for nursing students and practising nurses alike.
Overview of the Gall Bladder
Definition
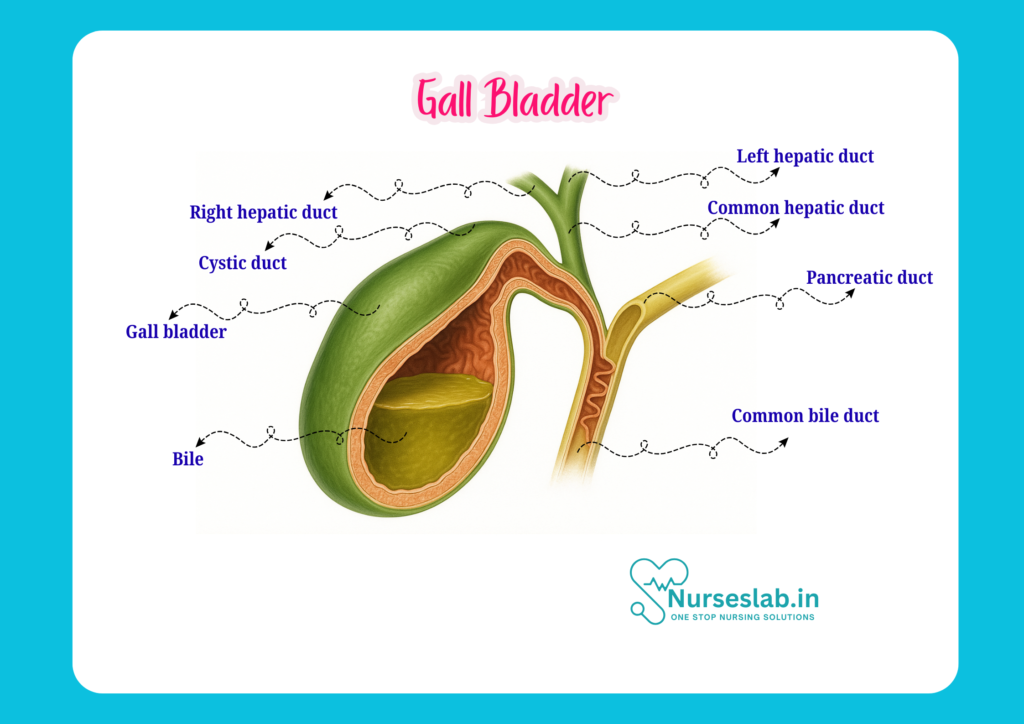
The gall bladder is a small, pear-shaped, hollow organ situated beneath the liver. Its primary role is to store and concentrate bile, a digestive fluid produced by the liver. The gall bladder releases bile into the small intestine to aid in the digestion of fats.
General Function
The gall bladder acts as a reservoir for bile. Between meals, it stores and concentrates bile by absorbing water and electrolytes. When fatty food enters the duodenum, the gall bladder contracts and ejects bile through the biliary tract into the intestine, facilitating fat emulsification and absorption.
Location and Relations
Anatomical Position
The gall bladder is located in the right upper quadrant of the abdomen, specifically in the fossa for the gall bladder on the visceral surface of the right lobe of the liver. It lies at the level of the ninth costal cartilage, where the right linea semilunaris meets the costal margin.
Neighbouring Organs
Understanding the anatomical relations of the gall bladder is essential, especially in surgical contexts and when interpreting clinical symptoms:
- Superiorly: Liver (specifically the right and quadrate lobes)
- Anteriorly: Anterior abdominal wall and the inferior surface of the liver
- Posteriorly: Transverse colon and the first and second parts of the duodenum
- Inferiorly: First part of the duodenum
- Medially: The porta hepatis and structures of the lesser omentum
The close proximity to these organs is clinically significant, as inflammation or enlargement of the gall bladder can affect or present with symptoms involving adjacent structures.
Structure of the Gall Bladder
Gross Structure
The gall bladder is a muscular, sac-like organ measuring about 7–10 cm in length and 3–4 cm in diameter. It typically has a capacity of 30–50 ml of bile.
Parts of the Gall Bladder
- Fundus: The rounded, blind end of the gall bladder, projecting beyond the inferior border of the liver. It is usually palpable when enlarged and lies opposite the tip of the ninth costal cartilage.
- Body: The main, largest part, tapering towards the neck. It lies against the visceral surface of the liver and is in contact with the transverse colon and the duodenum.
- Neck: The narrow, tapering portion that connects the body of the gall bladder to the cystic duct. The neck contains a spiral fold known as the valve of Heister, which helps regulate bile flow.
Layers of the Gall Bladder Wall
The gall bladder wall consists of the following layers, from inner to outer:
- Mucosa: Lined by simple columnar epithelium with microvilli, forming folds called rugae. The mucosa is highly absorptive.
- Muscularis: A layer of smooth muscle fibres arranged irregularly, responsible for contraction and bile expulsion.
- Perimuscular connective tissue: Contains blood vessels, lymphatics, and nerves.
- Serosa (adventitia): The outermost layer, a serous membrane derived from the peritoneum, covers the free surface. The surface attached to the liver is covered by connective tissue (adventitia) instead of serosa.
Blood Supply and Lymphatics
Arterial Supply
The gall bladder receives its blood supply primarily from the cystic artery, which commonly arises from the right hepatic artery. The cystic artery travels through the cystohepatic triangle (also known as Calot’s triangle), a key anatomical landmark during gall bladder surgery.
Venous Drainage
Venous blood from the gall bladder is drained by the cystic vein, which usually empties into the portal vein. Some smaller veins may drain directly into the liver substance (intrahepatic portal venous branches).
Lymphatic Drainage
Lymph from the gall bladder drains into the cystic lymph node (of Lund) located near the neck of the gall bladder. From there, lymph passes to the hepatic lymph nodes along the hepatic artery and eventually to the coeliac nodes. This lymphatic drainage pattern is significant in the spread of infection or malignancy.
Nerve Supply
Autonomic Innervation
The gall bladder is innervated by both sympathetic and parasympathetic fibres:
- Sympathetic nerves: Derived from the coeliac plexus, these fibres cause relaxation of the gall bladder and contraction of the sphincter of Oddi, inhibiting bile release during fasting.
- Parasympathetic nerves: Carried by the vagus nerve (cranial nerve X), they stimulate contraction of the gall bladder and relaxation of the sphincter of Oddi, promoting bile release during digestion.
- Sensory fibres: Travel with sympathetic nerves and are responsible for transmitting pain sensations, which can be referred to the right shoulder tip due to the phrenic nerve’s involvement.
Clinical Implications
Disorders of the gall bladder often present with pain in the right upper abdomen, sometimes radiating to the right shoulder or scapular region (referred pain). Understanding the nerve supply helps in interpreting these symptoms and in the administration of certain anaesthetic techniques.
Histology
Microscopic Structure
Under the microscope, the gall bladder displays unique histological features:
- Mucosa: The innermost layer consists of simple columnar epithelial cells with microvilli, specialised for absorption. The mucosa forms branching and interconnecting folds (rugae), increasing the surface area.
- Lamina propria: A layer of loose connective tissue beneath the epithelium, containing blood vessels and immune cells.
- Muscularis: A thin, discontinuous layer of smooth muscle fibres arranged in various directions. These muscle fibres contract to expel bile during digestion.
- Perimuscular connective tissue: Contains larger blood vessels, lymphatics, and nerves.
- Serosa or adventitia: The outermost covering. Where the gall bladder is attached to the liver, it is covered by adventitia; elsewhere, it is covered by peritoneal serosa.
Cell Types
The key cell type is the simple columnar epithelial cell with numerous microvilli, facilitating absorption of water and electrolytes. The absence of submucosa is a distinctive feature. Occasional mucous glands may be present near the neck of the gall bladder.
Functions of the Gall Bladder
The gall bladder plays several vital roles in digestion and overall health:
- Storage of bile: The liver continuously produces bile, which is stored in the gall bladder between meals.
- Concentration of bile: The gall bladder absorbs water and electrolytes from the stored bile, increasing its concentration and effectiveness in fat digestion.
- Release of bile: In response to the hormone cholecystokinin (released when fatty food enters the duodenum), the gall bladder contracts and releases concentrated bile into the duodenum via the cystic duct and common bile duct.
- Regulation of bile flow: The gall bladder coordinates with the sphincter of Oddi to regulate the timing and amount of bile entering the small intestine.
Clinical Relevance
Common Diseases of the Gall Bladder
- Cholelithiasis (Gall Stones): The formation of stones within the gall bladder, often composed of cholesterol or bilirubin. Stones can block the cystic duct or common bile duct, leading to pain, infection, or jaundice.
- Cholecystitis: Inflammation of the gall bladder, usually due to gall stones. Presents with right upper abdominal pain, fever, and sometimes jaundice.
- Gall bladder carcinoma: Malignancy of the gall bladder, more common in females and in regions with high rates of gall stones.
- Empyema and mucocele: Rare complications involving pus or mucus accumulation in the gall bladder.
- Biliary dyskinesia: Dysfunctional motility of the gall bladder, leading to biliary pain without stones.
Symptoms and Signs
Common symptoms of gall bladder disease include:
- Right upper abdominal pain (often after fatty meals)
- Nausea and vomiting
- Jaundice (yellowing of the skin and eyes)
- Fever (if infection is present)
- Referred pain to the right shoulder or back
Nursing Considerations
Nurses play a vital role in the care of patients with gall bladder disorders. Key responsibilities include:
- Assessment: Monitoring for signs of pain, jaundice, fever, and gastrointestinal symptoms.
- Pre-operative care: Preparing patients for imaging (ultrasound, CT scan) and surgery (laparoscopic or open cholecystectomy).
- Post-operative care: Observing for complications such as bleeding, infection, bile leak, or injury to adjacent organs. Educating patients about dietary modifications and the importance of follow-up.
- Patient education: Explaining the role of the gall bladder, the impact of its removal, and recognising symptoms that require urgent medical attention.
Role in Systemic Diseases
Gall bladder pathology can be associated with systemic diseases such as diabetes mellitus (increased risk of gall stones) and certain haemolytic disorders (pigment stones). Nurses must be aware of these associations in holistic patient assessment.
Summary and Key Points
- The gall bladder is a small, pear-shaped organ beneath the liver, essential for bile storage and concentration.
- It consists of the fundus, body, and neck, and is composed of mucosa, muscularis, connective tissue, and serosa/adventitia.
- Its blood supply is mainly from the cystic artery, and it drains into the portal vein and regional lymph nodes.
- Autonomic innervation (sympathetic and parasympathetic) regulates its contraction and relaxation.
- Histologically, it features a highly absorptive mucosa and lacks a submucosal layer.
- Gall bladder diseases include gall stones, cholecystitis, and cancer, all of which have significant clinical implications.
- Nurses must be adept at recognising symptoms, supporting treatments, and educating patients regarding gall bladder health.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.




