


Last Updated on July 10, 2026 by Nurseslab.in Editorial Team
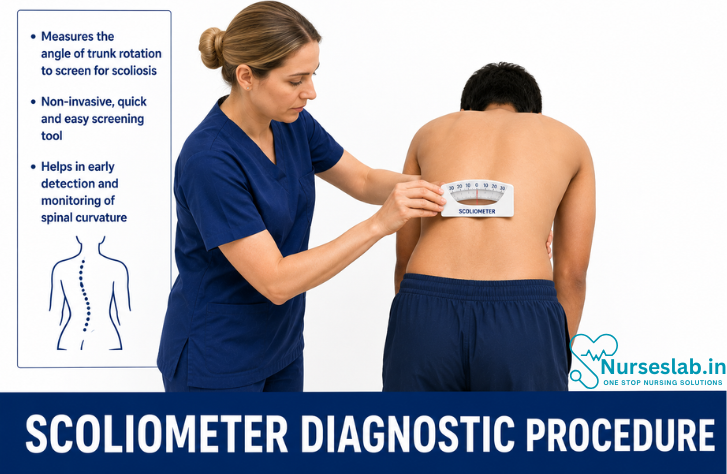
A scoliometer measures spinal curvature to screen for scoliosis, monitor progression, and support accurate musculoskeletal assessment in clinical and school settings.
Introduction
Scoliosis, a lateral curvature of the spine exceeding 10 degrees, is a prevalent musculoskeletal condition affecting individuals across age groups, particularly during the adolescent growth spurt. Early detection and appropriate management are crucial to prevent progression and associated complications. Among the various screening and diagnostic tools available, the scoliometer has emerged as a valuable, non-invasive instrument for the clinical assessment of scoliosis.
Purpose of Scoliometer Use
The scoliometer is primarily used in the clinical setting to quantify trunk asymmetry during forward bending tests, serving as an adjunct to physical examination for the detection and monitoring of scoliosis. Its main purposes include:
- Screening for scoliosis in asymptomatic individuals, especially adolescents.
- Assessing the degree of trunk rotation in patients with suspected or known scoliosis.
- Monitoring curve progression or response to treatment in follow-up visits.
- Guiding decisions on further imaging (e.g., spinal radiographs) or referral to specialists.
The scoliometer does not replace radiographic assessment but aids in identifying individuals who may benefit from further evaluation.
Equipment and Preparation
Description of the Scoliometer
A scoliometer is a handheld device, typically constructed of lightweight plastic, designed to measure the angle of trunk rotation (ATR) in degrees. The device resembles a spirit level with a central scale, usually ranging from 0 to 30 degrees, and a movable bubble or digital display indicating the measured angle. Some advanced models offer digital readouts or integration with smartphone applications, but the fundamental principle remains unchanged.
Patient Preparation
- Explain the purpose and process of the examination to the patient, addressing any concerns to ensure cooperation.
- Request the patient to remove upper body clothing to expose the spine and scapular region fully, maintaining privacy and comfort.
- Ensure the examination room is well-lit and the floor is flat to facilitate accurate assessment.
- Position the patient barefoot to avoid discrepancies caused by footwear.
Step-by-Step Diagnostic Procedure
The scoliometer assessment is most commonly performed in conjunction with the Adam’s Forward Bend Test. The following steps outline the standard procedure:
- Initial Inspection:
- Observe the patient from behind while standing naturally, noting any visible asymmetry of the shoulders, scapulae, or waist.
- Adam’s Forward Bend Test:
- Instruct the patient to stand with feet shoulder-width apart and knees straight.
- Ask the patient to bend forward at the waist, allowing the arms to hang freely with palms together, attempting to touch the toes.
- Ensure the head remains in line with the trunk, and the back is parallel to the floor.
- Scoliometer Placement:
- Identify the apex of the thoracic and/or lumbar curve visually or by palpation.
- Place the scoliometer horizontally across the back at the level of maximal rib or lumbar prominence (apex of the hump).
- Ensure the device is centred over the spinous processes for consistency.
- Measurement:
- Read the value indicated by the bubble (or digital display) on the scoliometer while keeping the device steady and parallel to the ground.
- Record the highest angle of trunk rotation (ATR) observed along the thoracic and lumbar regions separately.
- Repeat the measurement at adjacent spinal levels if necessary to identify the point of maximal rotation.
- Documentation:
- Record the ATR values, spinal levels, and any notable physical findings in the patient’s medical record.
Interpretation of Results
The scoliometer provides a quantitative measure of trunk rotation, expressed in degrees. The interpretation of these results is critical to guide subsequent clinical decisions:
- ATR less than 5 degrees:
- Generally considered within normal limits.
- No further immediate action required; advise routine monitoring if risk factors are present.
ATR between 5 and 7 degrees:
Suggests possible mild scoliosis.
Recommend closer clinical follow-up and repeat assessment at subsequent visits.
Consider radiographic evaluation if clinical suspicion remains high or if there are risk factors for progression.
ATR 7 degrees or greater:
Strongly suggestive of clinically significant scoliosis (typically correlates with a Cobb angle of 20 degrees or more on radiographs).
Referral for spinal radiographs and specialist evaluation is indicated.
It is important to note that the correlation between scoliometer readings and Cobb angle is not absolute; the scoliometer measures trunk rotation, not spinal curvature directly. Therefore, clinical judgement is essential in interpreting findings, particularly in borderline cases.
Clinical Significance
The scoliometer serves as a valuable tool in the early identification and monitoring of scoliosis, particularly in paediatric and adolescent populations. Its clinical significance lies in:
- Screening Efficiency: Enables rapid, non-invasive assessment of large populations, such as school-based screening programmes.
- Monitoring Progression: Facilitates tracking changes in trunk rotation over time, assisting in timely intervention.
- Reducing Unnecessary Radiographs: Helps identify individuals who require imaging, thus minimising radiation exposure in low-risk cases.
- Referral Criteria: Aids in determining when specialist referral or further diagnostic work-up is warranted.
Appropriate use of the scoliometer can contribute significantly to the optimisation of scoliosis management pathways, ensuring that resources are directed towards individuals most likely to benefit from intervention.
Limitations and Considerations
While the scoliometer is a useful adjunct in clinical practice, several limitations and considerations must be acknowledged:
- Operator Dependence: Accurate measurement requires correct positioning and technique. Inter- and intra-observer variability can affect reliability.
- Patient Factors: Body habitus, muscle bulk, and spinal flexibility may influence readings. Obesity or significant muscular development can obscure spinal landmarks.
- Measurement Specificity: The scoliometer quantifies trunk rotation, not spinal curvature. It may not detect non-rotational or early-stage curves.
- False Positives/Negatives: Conditions such as leg length discrepancy or postural asymmetry may yield abnormal readings in the absence of true scoliosis.
- Not a Standalone Diagnostic Tool: The scoliometer should be used in conjunction with a comprehensive clinical assessment, not as a sole basis for diagnosis or management decisions.
Awareness of these limitations is essential to avoid misinterpretation and ensure the appropriate application of findings.
Best Practices
To maximise the utility and accuracy of the scoliometer in clinical settings, adherence to best practices is recommended:
- Standardise Technique: Ensure all examiners are trained in the correct use of the scoliometer, including patient positioning and device placement.
- Consistent Positioning: Always position the patient and the scoliometer in the same manner at each assessment to facilitate reliable comparisons over time.
- Multiple Measurements: Record readings at several points along the spine to identify the maximal ATR and improve diagnostic accuracy.
- Comprehensive Documentation: Note ATR values, spinal level, patient positioning, and any relevant clinical findings in the medical record.
- Use in Context: Integrate scoliometer findings with the patient’s history, physical examination, and risk factors before making management decisions.
- Follow-up and Referral: Establish clear protocols for follow-up, repeat assessments, and referral criteria based on ATR thresholds and clinical context.
- Maintain Equipment: Regularly check and calibrate the scoliometer, especially if using digital models, to ensure ongoing accuracy.
Incorporating these best practices enhances the reliability of the scoliometer as a screening and monitoring tool for scoliosis.
Nursing Care of Patients Undergoing Scoliometer Assessment
Effective nursing care encompasses preparation, patient education, procedural assistance, infection control, emotional support, thorough documentation, and diligent post-assessment care. By adopting a holistic and patient-centred approach, nurses contribute significantly to early detection, timely intervention, and ongoing patient support.
Pre-Assessment Preparation
Before commencing a scoliometer assessment, comprehensive preparation is essential to facilitate a smooth and accurate procedure. The nurse should begin by reviewing the patient’s medical history, including any previous diagnoses of spinal conditions, family history of scoliosis, and current symptoms or complaints. This review helps tailor the approach to the individual’s needs and identifies any contraindications or factors that may influence the assessment process.
Equipment readiness is equally important. All necessary tools—scoliometer, disposable gloves, cleaning agents, and documentation materials—must be gathered and checked for functionality, cleanliness, and calibration. The nurse should verify the device’s accuracy to avoid measurement errors. The assessment area should be set up to ensure patient comfort, privacy, and adequate lighting. For paediatric and adolescent patients, additional considerations such as a guardian’s presence and child-friendly explanations may be necessary to alleviate anxiety.
Patient Education and Communication
Clear and compassionate communication is a cornerstone of effective nursing care. The nurse should explain the purpose of the scoliometer assessment, the steps involved, and what the patient can expect during the procedure. It is vital to use language appropriate for the patient’s age, comprehension level, and cultural background. Visual aids or models can be particularly helpful when educating children or adolescents.
Obtaining informed consent is a legal and ethical requirement. For adults, this involves direct discussion with the patient, while for minors, parental or guardian consent must be obtained. The nurse should encourage questions, address any concerns, and reassure the patient of confidentiality and privacy. This process fosters trust and cooperation, which are essential for accurate assessment results.
Procedural Support
During the assessment, the nurse plays an active role in guiding the patient through each step. Proper positioning is critical; the nurse should assist the patient in standing upright with feet shoulder-width apart and arms at the sides. For the Adam’s Forward Bend Test, clear instructions and gentle physical guidance may be required, especially for younger patients, to ensure the back is parallel to the floor and the arms hang freely.
Throughout the procedure, the nurse should monitor the patient’s comfort and physical response. If the patient exhibits signs of discomfort, dizziness, or anxiety, the nurse must pause, provide reassurance, and adjust the approach as needed. For paediatric patients, distraction techniques such as conversation or allowing a parent to be present can be beneficial. Adult patients may appreciate a calm, professional demeanour and detailed explanations to reduce apprehension.
Infection Control Measures
Strict adherence to infection control protocols protects both patients and healthcare providers. The nurse should perform hand hygiene before and after the assessment, using soap and water or an alcohol-based hand rub. Gloves should be worn if there is a risk of contact with body fluids or if the patient has open skin lesions. All equipment, including the scoliometer, must be cleaned and disinfected between uses to prevent cross-contamination.
Using disposable sheets or covers can further reduce infection risks, especially in settings where multiple patients are assessed in succession. The nurse should also be attentive to the patient’s personal hygiene and dignity, ensuring that exposure is minimised and privacy is maintained at all times.
Emotional and Psychological Support
Undergoing a physical assessment can be a source of anxiety, particularly for children, adolescents, and individuals undergoing the procedure for the first time. The nurse should adopt a supportive and empathetic approach, providing reassurance and normalising the experience. Maintaining a calm and friendly environment helps to reduce fear and fosters cooperation.
For paediatric patients, involving parents or guardians and using age-appropriate communication are crucial. Adolescents may require additional privacy and sensitivity to body image concerns. Adult patients may benefit from being informed about the relevance of the assessment and having their questions answered in detail. In all cases, upholding the patient’s dignity, offering choices when possible, and encouraging open dialogue contribute to a positive experience.
Documentation and Reporting
Accurate and thorough documentation is a professional responsibility and is essential for continuity of care. The nurse should record the findings of the scoliometer assessment, including the angle of trunk rotation, the side of deviation, and any observations regarding posture or mobility. Any patient-reported symptoms or concerns should also be documented.
If abnormal findings are detected, the nurse should promptly communicate these to the attending physician or relevant healthcare team members for further evaluation and management. Documentation should be completed immediately after the assessment to ensure accuracy and to provide a clear record for future reference.
Post-Assessment Care
Following the assessment, the nurse should guide the patient on the next steps, which may include further diagnostic testing, referral to a specialist, or routine monitoring. The nurse should provide clear instructions based on the assessment findings and respond to any remaining questions or concerns. For paediatric and adolescent patients, this may involve discussing the results with parents or guardians and providing written information or resources.
The nurse should also assess the patient’s emotional state post-procedure, offering reassurance and support as needed. In cases where the assessment has revealed potential abnormalities, the nurse should explain the implications in a sensitive manner and outline the follow-up process, emphasising that early detection is key to effective management.
Special Considerations: Paediatric, Adolescent, and Adult Patient Needs
Nursing care must be tailored to the unique needs of each age group. For paediatric patients, the presence of a familiar adult, use of play, and positive reinforcement are effective strategies. Adolescents may benefit from greater autonomy, privacy, and assurance that their concerns are taken seriously. Adult patients often value clear explanations, involvement in decision-making, and respect for their preferences and dignity.
Cultural sensitivity is also important, as beliefs and attitudes towards medical procedures can vary. The nurse should remain flexible and adapt communication and care strategies to suit individual backgrounds and expectations, ensuring equitable and respectful care for all patients.
Conclusion: Nursing Responsibilities and Patient-Centred Care
The role of the nurse in scoliometer assessment extends far beyond technical execution. By integrating thorough preparation, effective communication, procedural support, stringent infection control, emotional reassurance, meticulous documentation, and comprehensive post-assessment care, nurses uphold the highest standards of patient-centred practice. Tailoring care to the developmental stage and unique needs of paediatric, adolescent, and adult patients ensures not only accurate assessment outcomes but also a positive and supportive experience for every individual. In doing so, nurses play a pivotal role in the early detection and holistic management of scoliosis, ultimately contributing to better health outcomes and enhanced patient well-being.
REFERENCES
- Gerard L. Glancy, Advances in Idiopathic Scoliosis in Children and Adolescents, Advances in Pediatrics,Volume 54, Issue 1,2007,Pages 55-66,ISSN 0065-3101,https://doi.org/10.1016/j.yapd.2007.03.005. https://www.sciencedirect.com/science/article/pii/S0065310107000060)
- American Academy of Orthopaedic Surgeons. Introduction to Scoliosis (https://orthoinfo.aaos.org/en/diseases–conditions/introduction-to-scoliosis/).
- Kuznia AL, Hernandez AK, Lee LU. Adolescent Idiopathic Scoliosis: Common Questions and Answers https://pubmed.ncbi.nlm.nih.gov/31894928/). Am Fam Physician. 2020 Jan 1;101(1):19-23.
- MedlinePlus. Scoliosis (https://medlineplus.gov/ency/article/001241.htm).
- Radiopaedia. Cobb angle (https://radiopaedia.org/articles/cobb-angle?lang=us).
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.


