


Last Updated on May 27, 2026 by Nurseslab.in Editorial Team
The small intestine is a vital component of the human digestive system, playing a central role in digestion and nutrient absorption.
Introduction
Nurses are frequently involved in the care of patients with gastrointestinal conditions, surgical interventions, and nutritional issues. A solid grasp of the anatomy and physiology of the small intestine equips nurses to better understand symptoms, anticipate complications, administer appropriate interventions, and provide holistic care.
General Overview of the Small Intestine
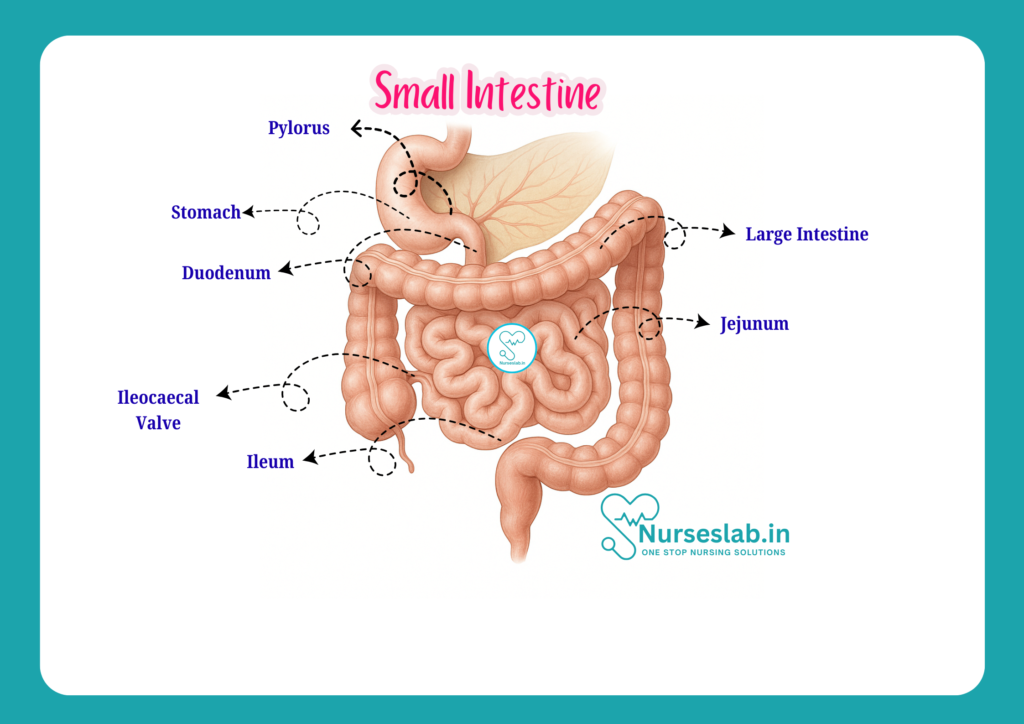
The small intestine is a long, coiled tube that extends from the stomach to the large intestine. It is the principal organ for digestion and absorption of nutrients. In adults, the small intestine measures approximately 6 metres (about 20 feet) in length, although it can range from 4.5 to 7 metres depending on individual factors. The small intestine occupies a significant portion of the abdominal cavity, being loosely arranged in the central and lower parts.
Its primary functions include:
- Completing the digestion of food using enzymes and bile
- Absorbing nutrients, electrolytes, and water into the bloodstream
- Facilitating immune surveillance through gut-associated lymphoid tissue (GALT)
The small intestine is divided into three main segments: the duodenum, jejunum, and ileum, each with distinctive anatomical and functional characteristics.
Divisions of the Small Intestine
Duodenum
The duodenum is the first and shortest segment of the small intestine, measuring about 25 cm (10 inches) in length. It forms a C-shaped curve around the head of the pancreas and lies primarily in the upper abdomen, retroperitoneally (behind the peritoneum).
Structural Parts of the Duodenum:
- Superior (First) Part: Begins at the pylorus of the stomach and runs horizontally to the right. It is the most mobile section and is intraperitoneal for the initial 2.5 cm (duodenal cap or bulb).
- Descending (Second) Part: Runs vertically downward, receiving the common bile duct and pancreatic duct at the major duodenal papilla (important for bile and pancreatic juice entry).
- Horizontal (Third) Part: Passes horizontally across the inferior vena cava and aorta.
- Ascending (Fourth) Part: Ascends to the left of the aorta to join the jejunum at the duodenojejunal flexure, supported by the ligament of Treitz.
Relations: The duodenum is closely related to the pancreas, gallbladder, liver, right kidney, and major blood vessels, making it clinically significant in cases of trauma, ulcers, or tumours.
Jejunum
The jejunum is the middle segment, comprising roughly the upper two-fifths of the remaining small intestine after the duodenum. It is about 2.5 metres (8 feet) long and is located mainly in the left upper quadrant of the abdomen.
Features of the Jejunum:
- Thicker wall and larger diameter compared to the ileum
- More prominent mucosal folds (plicae circulares)
- Greater vascularity (appears redder)
- Less fat in the mesentery (the fold of tissue that attaches the intestine to the posterior abdominal wall)
The jejunum is primarily responsible for the absorption of carbohydrates, proteins, and the majority of water-soluble vitamins.
Ileum
The ileum forms the final three-fifths of the small intestine (about 3.5 metres or 12 feet long) and ends at the ileocaecal junction, where it meets the large intestine (caecum).
Features of the Ileum:
- Thinner wall, smaller diameter than the jejunum
- Fewer and less prominent mucosal folds
- More fat in the mesentery
- Pale pink appearance due to less vascularity
- Presence of Peyer’s patches—aggregated lymphoid nodules important for immune function
The terminal ileum is especially significant for the absorption of vitamin B12 and bile salts, which are crucial for red blood cell production and fat digestion, respectively.
Histology of the Small Intestine
The wall of the small intestine is composed of four main layers, each contributing to its specialised functions:
Mucosa:
- Inner lining, highly folded to increase surface area
- Contains villi (finger-like projections) and microvilli (microscopic projections on enterocytes), forming the ‘brush border’ for enhanced absorption

Epithelium includes several cell types:
- Enterocytes: Main absorptive cells, rich in enzymes
- Goblet Cells: Secrete mucus for lubrication and protection
- Paneth Cells: Located at the base of crypts, produce antimicrobial peptides
- Enteroendocrine Cells: Secrete hormones (e.g., secretin, cholecystokinin) regulating digestion
- Lamina propria (connective tissue) and muscularis mucosae (thin muscle layer) support the epithelium
Submucosa:
- Connective tissue layer containing blood vessels, lymphatics, and nerves (Meissner’s plexus)
- Brunner’s glands (in duodenum) secrete alkaline mucus to neutralise gastric acid
Muscularis externa:
- Two layers of smooth muscle—inner circular and outer longitudinal
- Responsible for peristalsis and segmentation movements
- Contains Auerbach’s (myenteric) plexus for motor control
Serosa (or Adventitia):
- Outermost layer, a thin membrane (serosa) covers most of the small intestine except for the retroperitoneal duodenum (adventitia)
Differences Along the Small Intestine:
- Duodenum: Presence of Brunner’s glands; few villi
- Jejunum: Tall, numerous villi and plicae circulares; no Brunner’s glands
- Ileum: Shorter villi; prominent Peyer’s patches (lymphoid tissue)
Blood Supply
A rich blood supply is critical for the small intestine’s absorptive and metabolic activities.
Arterial Supply
The main arterial supply to the small intestine comes from the superior mesenteric artery (SMA), a major branch of the abdominal aorta.
- Duodenum: Supplied by branches of both the celiac trunk (via the superior pancreaticoduodenal artery) and the SMA (via the inferior pancreaticoduodenal artery)
- Jejunum and Ileum: Supplied by multiple jejunal and ileal branches of the SMA, which form arcades (loops) and vasa recta (straight arteries) within the mesentery
Venous Drainage
Venous blood from the small intestine drains into the superior mesenteric vein, which eventually joins the splenic vein to form the portal vein, directing nutrient-rich blood to the liver for processing.
Clinical Relevance
- Ischaemia: Sudden blockage of the SMA can lead to acute mesenteric ischaemia, a life-threatening condition requiring emergency intervention
- Bleeding: Gastrointestinal bleeding from ulcers or vascular malformations in the small intestine may present as melena or obscure GI bleeding
Nerve Supply
The small intestine’s activity is regulated by both the autonomic nervous system (ANS) and the local enteric nervous system (ENS).
Autonomic Innervation
- Sympathetic fibres: Arise from the thoracic spinal cord (T5–T12), synapse in the superior mesenteric ganglion, and inhibit intestinal motility and secretion
- Parasympathetic fibres: Provided mainly by the vagus nerve, stimulate peristalsis and glandular secretion
Enteric Nervous System
The ENS comprises two main plexuses:
- Myenteric (Auerbach’s) plexus: Located between the muscle layers, controls muscular contractions
- Submucosal (Meissner’s) plexus: Regulates secretions and blood flow
Clinical Implications
- Disorders of gut motility, such as paralytic ileus or pseudo-obstruction, may arise from nerve damage or dysfunction
- Autonomic neuropathy in diabetes can impair intestinal function, leading to symptoms like diarrhoea or constipation
Lymphatic Drainage
Lymphatic vessels in the small intestine are essential for transporting absorbed fats and immune defence.
- Lacteals: Specialised lymphatic capillaries within villi absorb dietary fats as chylomicrons
- Mesenteric Lymph Nodes: Lymph from the intestine drains through a series of nodes along the mesentery before reaching the cisterna chyli and thoracic duct
Clinical Significance
- Malignancy: Cancers of the small intestine or adjacent organs can spread via lymphatic channels to mesenteric nodes
- Infection: Bacterial or parasitic infections may cause lymphadenitis (inflammation of lymph nodes), contributing to abdominal pain and systemic symptoms
Functions of the Small Intestine
The small intestine is the main site for digestion and absorption of nutrients. Its key functions include:
- Digestion: Enzymes from the pancreas (proteases, lipases, amylases) and bile from the liver work within the duodenum to break down proteins, fats, and carbohydrates into absorbable units.
- Absorption: The extensive surface area provided by villi and microvilli enables rapid absorption of:
- Monosaccharides (glucose, galactose, fructose)
- Amino acids and small peptides
- Fatty acids, glycerol, and monoglycerides (as micelles and chylomicrons)
- Vitamins and minerals (notably iron, calcium, and B12)
- Water and electrolytes
- Immune Functions: The gut-associated lymphoid tissue (GALT), including Peyer’s patches, provides immune surveillance, producing immunoglobulins and responding to pathogens.
Clinical Relevance
An understanding of the small intestine’s anatomy is crucial for recognising, diagnosing, and managing various clinical conditions. Some of the most common and significant include:
- Crohn’s Disease: A chronic inflammatory bowel disease that often affects the terminal ileum, causing ulcers, strictures, and fistulas. Symptoms include abdominal pain, diarrhoea, weight loss, and malnutrition. Nursing care involves monitoring for complications, supporting nutrition, and assisting with medication adherence.
- Coeliac Disease: An autoimmune disorder where ingestion of gluten damages the small intestinal mucosa, leading to villous atrophy and malabsorption. Nurses play a key role in patient education, dietary management, and monitoring for complications.
- Intestinal Obstruction: May result from adhesions, tumours, hernias, or volvulus. Presents with abdominal pain, vomiting, and constipation. Early identification and prompt intervention are vital to prevent ischaemia and perforation.
- Short Bowel Syndrome: Occurs after significant surgical resection, resulting in malabsorption and nutritional deficiencies. Management includes nutritional support, medication, and patient education.
- Infections and Infestations: Bacterial, viral, or parasitic infections can cause enteritis, diarrhoea, and dehydration—conditions requiring vigilant nursing assessment and supportive care.
- Surgical Considerations: Procedures such as resections, stoma formation, or anastomoses require knowledge of intestinal anatomy for preoperative and postoperative care, wound management, and monitoring for complications such as leakage, infection, or bowel obstruction.
Nursing Care Points:
- Monitor for signs of malabsorption (weight loss, anaemia, steatorrhoea)
- Assess for abdominal pain, distension, and changes in bowel habits
- Support patients with dietary modifications as advised by the dietician or medical team
- Educate patients and families about disease processes, medication adherence, and signs of complications
- Collaborate with multidisciplinary teams for holistic care
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.



