


Last Updated on May 28, 2026 by Nurseslab.in Editorial Team
Introduction
Understanding the anatomy of the urinary bladder is fundamental for nurses and nursing students. As frontline healthcare providers, nurses encounter conditions related to the urinary bladder in various clinical settings—from routine care to emergency interventions. A thorough knowledge of the bladder’s structure, location, and function aids in patient assessment, catheterisation, monitoring, and education.
Overview of the Urinary Bladder
Definition
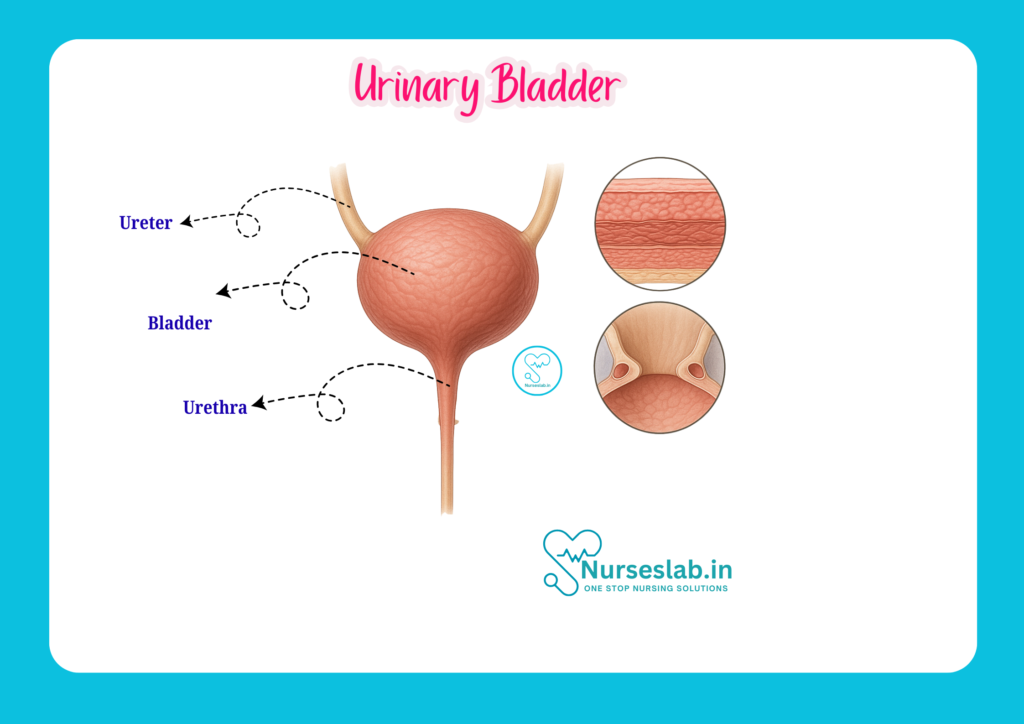
The urinary bladder is a hollow, muscular organ situated in the pelvic cavity. Its primary function is to store urine produced by the kidneys before it is excreted from the body. The bladder is a crucial component of the urinary system, which also includes the kidneys, ureters, and urethra.
Function and Role in the Urinary System
The bladder’s main role is to act as a reservoir for urine, allowing for controlled and intermittent urination. It receives urine from the kidneys via the ureters and expels it through the urethra during the process of micturition (urination). The bladder’s ability to expand and contract is vital for maintaining urinary continence and ensuring proper elimination of waste.
Location and Relations
Anatomical Position
The urinary bladder is located in the lesser pelvis, posterior to the pubic symphysis. Its position varies depending on whether it is empty or full. When empty, it lies entirely within the pelvis; as it fills, it rises into the lower abdomen.
Relations to Surrounding Organs
The anatomical relations of the bladder differ between males and females, which is essential for nurses to understand during patient care and procedures.
- In Males: The bladder lies anterior to the rectum and superior to the prostate gland. The seminal vesicles and vas deferens are positioned posterior and inferior to the bladder.
- In Females: The bladder is situated anterior to the uterus and upper part of the vagina. It is separated from the rectum by the uterus and the posterior vaginal wall.
Superiorly, the bladder is loosely covered by peritoneum, while inferiorly, it rests on the pelvic floor muscles. Laterally, it is bordered by the obturator internus muscles and the pelvic side walls.
External Features of the Urinary Bladder
The urinary bladder has distinct external features that are vital for clinical identification and understanding its function.
Shape
In an empty state, the bladder is tetrahedral (pyramidal) in shape; when full, it becomes more ovoid and rounded.
Surfaces
The bladder presents with several surfaces:
- Superior (dome) surface: Covered by peritoneum, faces upward and slightly backward.
- Inferolateral surfaces (right and left): In contact with pelvic floor muscles and the obturator internus.
- Posterior surface (base or fundus): Faces downward and backward; in males, it is related to the rectum, seminal vesicles, and vas deferens; in females, it is related to the anterior wall of the vagina and cervix.
Apex
The apex is the anterior pointed end of the bladder, which is attached to the umbilicus by the median umbilical ligament (a remnant of the urachus).
Base (Fundus)
The base or fundus is the posterior surface, which is broad and fixed. It is important in clinical examination and imaging.
Neck
The neck of the bladder is the lowest and most fixed part, located where the bladder joins the urethra. In males, it is surrounded by the prostate gland; in females, it is closely related to the pelvic floor.
Fundus
The fundus is often used interchangeably with the base but typically refers to the broad, posterior aspect of the bladder.
Internal Structure of the Urinary Bladder
Mucosa
The innermost lining of the bladder is the mucosa, which is highly folded (forming rugae) when the bladder is empty. These folds allow the bladder to expand as it fills. The mucosa is smooth at the trigone area, even when the bladder is empty.
Muscular Layers (Detrusor Muscle)
Beneath the mucosa lies the detrusor muscle, a thick coat of smooth muscle fibres arranged in three layers: inner longitudinal, middle circular, and outer longitudinal. The detrusor muscle contracts during micturition to expel urine.
Trigone
The trigone is a triangular, smooth area at the base of the bladder, delineated by the two ureteric orifices (where the ureters enter the bladder) and the internal urethral orifice. Unlike the rest of the bladder, the trigone is firmly attached to the underlying muscle and lacks rugae, making it clinically significant as a common site for infections and tumours.
Lining Epithelium
The bladder is lined by transitional epithelium, also known as urothelium. This specialised lining allows the bladder to stretch and maintain a barrier against urine constituents.
Histology of the Urinary Bladder
A microscopic examination of the bladder reveals several distinct layers:
- Mucosa: Composed of transitional epithelium (urothelium), which appears as multiple layers of cells that can change shape depending on the degree of bladder distension. The underlying lamina propria contains connective tissue, blood vessels, and nerves.
- Submucosa: In the bladder, the submucosa is not well defined, as the lamina propria blends with the muscular layer.
- Muscularis (Detrusor Muscle): Made up of three interlacing layers of smooth muscle, responsible for the contractile function of the bladder.
- Adventitia/Serosa: The outermost covering is adventitia (connective tissue) on the inferior and lateral parts, while the superior surface is covered by serosa (peritoneum).
Blood Supply of the Urinary Bladder
Arterial Supply
The bladder receives blood primarily from branches of the internal iliac arteries:
- Superior vesical arteries: Supply the upper part of the bladder.
- Inferior vesical arteries (in males): Supply the lower part of the bladder, prostate, and seminal vesicles.
- Vaginal arteries (in females): The equivalent of the inferior vesical arteries, supplying the lower bladder and adjacent structures.
Venous Drainage
Venous blood from the bladder drains into the vesical venous plexus, which surrounds the bladder and communicates with the prostatic (in males) or uterovaginal (in females) venous plexuses. These eventually drain into the internal iliac veins.
Nerve Supply of the Urinary Bladder
The bladder’s nerve supply is complex, involving both autonomic (sympathetic and parasympathetic) and sensory (afferent) fibres, which regulate storage and voiding of urine.
Autonomic Nerve Supply
- Sympathetic fibres: Originate from the T11–L2 spinal segments and reach the bladder via the hypogastric plexus. They primarily facilitate urine storage by relaxing the detrusor muscle and contracting the internal urethral sphincter.
- Parasympathetic fibres: Arise from the S2–S4 spinal segments and travel through the pelvic splanchnic nerves. They stimulate contraction of the detrusor muscle and relaxation of the internal sphincter, promoting micturition.
Sensory (Afferent) Nerve Supply
Afferent fibres convey sensations of bladder fullness and pain. These fibres travel with both sympathetic and parasympathetic pathways to the spinal cord.
Lymphatic Drainage
The lymphatic drainage of the bladder is clinically significant, especially in the spread of infections and malignancies.
- Primary lymphatic drainage: Lymph from the bladder drains into the external iliac, internal iliac, and sacral lymph nodes.
- Clinical significance: Knowledge of lymphatic drainage pathways is important in the staging and management of bladder cancer, as well as in understanding the spread of pelvic infections.
Developmental Aspects
Embryological Development
The urinary bladder develops from the urogenital sinus, which is part of the cloaca in the early embryo. The upper part of the bladder is derived from the vesical part of the urogenital sinus, while the trigone area is formed by the incorporation of the caudal ends of the mesonephric ducts. The urachus, a remnant of the allantois, forms the median umbilical ligament after birth.
Congenital Anomalies
Some congenital anomalies related to the bladder include:
- Exstrophy of the bladder: A rare condition where the anterior wall of the bladder and the overlying abdominal wall fail to develop, exposing the bladder mucosa.
- Persistent urachus (patent urachus): The urachus fails to close, resulting in a communication between the bladder and the umbilicus, which may cause urine leakage from the umbilicus.
- Vesicoureteral reflux: An abnormal backflow of urine from the bladder into the ureters, increasing the risk of infections.
Clinical Relevance
Common Conditions Affecting the Bladder
- Urinary Tract Infection (UTI): The bladder is frequently involved in UTIs, particularly in females due to their shorter urethra. Symptoms include dysuria (painful urination), frequency, urgency, and suprapubic discomfort.
- Cystitis: Inflammation of the bladder, often due to infection. Cystitis can be acute or chronic and may present with similar symptoms as UTIs.
- Bladder Stones: Crystalline deposits may form in the bladder, leading to pain, haematuria (blood in urine), and recurrent infections.
- Bladder Tumours: Both benign and malignant tumours can arise from the bladder epithelium, with transitional cell carcinoma being the most common malignancy.
Catheterisation and Nursing Considerations
Catheterisation is the process of inserting a tube through the urethra into the bladder to drain urine. It is a common nursing procedure, especially for patients with urinary retention, during surgery, or when accurate urine output measurement is required. Nurses must be familiar with the anatomy of the bladder and urethra to perform catheterisation safely, prevent infections, and monitor for complications such as trauma or blockage.
Nurses should also be aware of the signs and symptoms of bladder dysfunction, including incontinence, retention, and suprapubic pain. Prompt recognition and appropriate intervention can prevent complications and improve patient outcomes.
Other Clinical Procedures and Interventions
- Bladder irrigation: Used to clear blood clots or debris post-surgery or in cases of haematuria.
- Cystoscopy: Endoscopic examination of the bladder, useful in diagnosing tumours, stones, and other pathologies.
- Suprapubic catheterisation: Involves placing a catheter directly into the bladder through the abdominal wall, usually when the urethral route is not possible.
Summary: Key Takeaways for Nursing Practice
- The urinary bladder is a muscular, hollow organ essential for urine storage and controlled release.
- Understanding its anatomy, including location, relations, and internal structure, is crucial for safe nursing care.
- Knowledge of blood supply, nerve supply, and lymphatic drainage aids in recognising and managing bladder diseases.
- Developmental aspects and congenital anomalies should be considered in paediatric and congenital cases.
- Clinical relevance includes common conditions like UTIs, cystitis, bladder stones, tumours, and the importance of correct catheterisation technique.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.



