


Last Updated on May 28, 2026 by Nurseslab.in Editorial Team
Understanding the anatomy of the ureter is fundamental for nurses, as it equips them with the knowledge needed to assess, monitor, and care for patients with urinary tract conditions. The ureter, a crucial component of the urinary system, is often involved in various clinical scenarios, from urinary tract infections to kidney stones.
Overview of the Urinary System
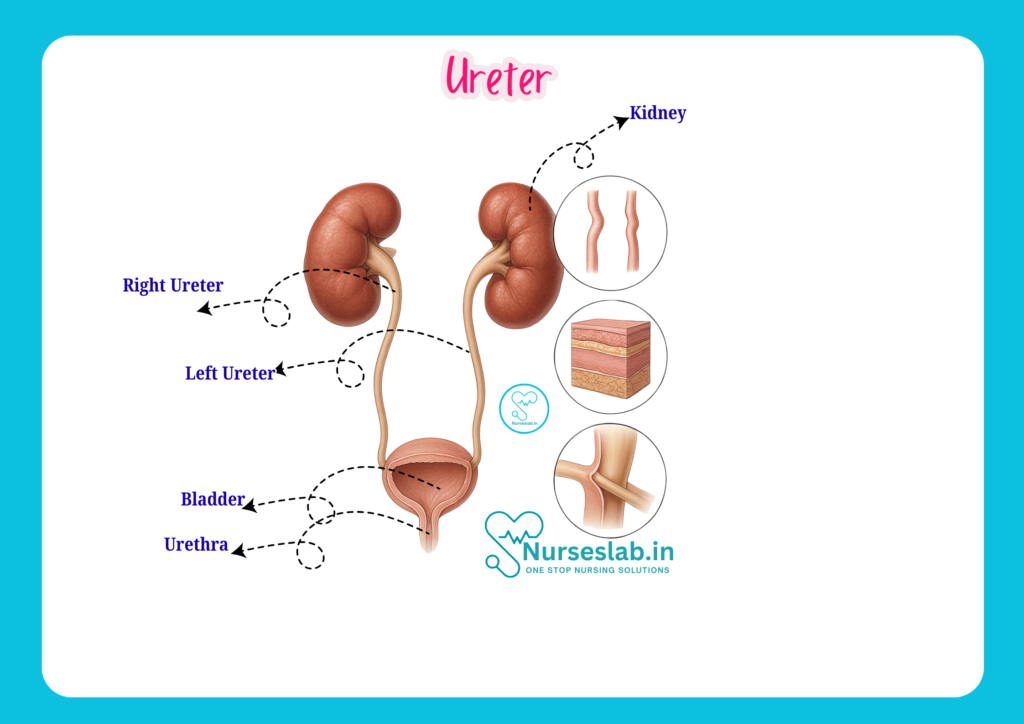
The urinary system, also known as the renal system, is responsible for the production, storage, and excretion of urine. It comprises the kidneys, ureters, urinary bladder, and urethra. Each organ plays a unique role in maintaining fluid and electrolyte balance, removing metabolic waste, and regulating blood pressure. The ureter specifically acts as the conduit, transporting urine from the kidneys to the bladder, ensuring the efficient elimination of waste products from the body.
Gross Anatomy of the Ureter
Definition and Basic Structure
The ureter is a paired, muscular tube that conveys urine from each kidney to the urinary bladder. There are two ureters in the human body, one arising from each kidney. They are retroperitoneal structures, meaning they lie behind the peritoneum, the lining of the abdominal cavity.
Length and Dimensions
Each ureter typically measures about 25–30 cm in length and 3–4 mm in diameter in adults. The length can vary depending on an individual’s height and other anatomical factors. The ureter is slightly longer in males than in females due to the differences in pelvic anatomy.
Location and Course
The ureter begins at the renal pelvis, which is the funnel-shaped upper end of the ureter located at the hilum of the kidney. From here, it descends vertically downwards along the posterior abdominal wall. The course of the ureter can be divided into two parts:
- Abdominal Part: This segment extends from the renal pelvis to the pelvic brim. It runs downwards and medially, lying on the psoas major muscle, and crosses the common iliac vessels at the pelvic brim.
- Pelvic Part: After crossing into the pelvis, the ureter travels downwards and forwards along the lateral pelvic wall before entering the urinary bladder at its posterolateral aspect.
Anatomical Relations
Understanding the anatomical relations of the ureter is vital for nurses, especially when considering surgical procedures, catheterisation, or the spread of infections. Key relations include:
- Posteriorly: The ureter is related to the psoas major muscle and the tips of the transverse processes of the lumbar vertebrae.
- Anteriorly: In the abdomen, the right ureter is crossed by the duodenum, gonadal vessels, and right colic vessels, while the left ureter is related to the left colic vessels and sigmoid mesocolon.
- In the Pelvis: In males, the ureter passes beneath the vas deferens and near the seminal vesicles. In females, it passes close to the uterine artery (“water under the bridge” – a key landmark during gynaecological surgery).
Constrictions of the Ureter
There are three natural constrictions along the course of the ureter, which are clinically significant as they are common sites for the impaction of ureteric stones:
- At the pelvi-ureteric junction (where the renal pelvis narrows to become the ureter)
- Where the ureter crosses the pelvic brim (over the iliac vessels)
- At the vesico-ureteric junction (where the ureter enters the bladder wall)
Histological Structure of the Ureter
The histology of the ureter is essential knowledge for nurses, as it explains the tube’s physiological functions and responses to disease. The ureter is composed of three main layers:
Mucosa
The innermost layer is the mucosa, which lines the lumen of the ureter. The mucosa consists of:
- Transitional Epithelium (Urothelium): This unique epithelium allows the ureter to stretch as urine passes through. It is composed of several layers of cells that can change shape from cuboidal to squamous, providing a flexible yet protective lining.
- Lamina Propria: A connective tissue layer beneath the epithelium, rich in blood vessels, nerves, and lymphatics.
Muscularis
The muscularis is a thick layer of smooth muscle responsible for the peristaltic contractions that propel urine towards the bladder. It is arranged in two main sublayers:
- Inner Longitudinal Muscle Layer
- Outer Circular Muscle Layer
In the lower third of the ureter, an additional outer longitudinal layer is present, enhancing the strength of peristaltic waves as urine approaches the bladder.
Adventitia
The outermost layer, the adventitia, is composed of connective tissue containing blood vessels, nerves, and lymphatics. It anchors the ureter to surrounding structures and provides structural support.
Functional Relevance of Histological Layers
Each histological layer plays a vital role in the function of the ureter:
- The transitional epithelium protects underlying tissues from urine’s toxic effects and accommodates volume changes.
- The muscularis generates peristaltic waves, ensuring unidirectional urine flow.
- The adventitia maintains the ureter’s position and acts as a conduit for neurovascular supply.
Blood Supply of the Ureter
Arterial Supply
The arterial supply to the ureter is segmental and comes from multiple sources along its course:
- Upper third: Supplied by branches from the renal arteries.
- Middle third: Receives blood from the gonadal arteries (testicular or ovarian) and the aorta.
- Lower third: Supplied by branches of the common iliac, internal iliac, and superior vesical arteries.
These arteries form a longitudinal anastomosis along the ureter, ensuring a rich blood supply even if one source is compromised.
Venous Drainage
The venous drainage of the ureter closely follows its arterial supply:
- Upper third: Drains into the renal veins.
- Middle third: Drains into the gonadal veins.
- Lower third: Drains into the internal iliac and vesical veins.
Clinical Implications of Blood Supply
Knowledge of the segmental blood supply is crucial during surgical procedures such as ureteric reimplantation or when dealing with trauma to avoid ischaemia and subsequent stricture formation. Compromised blood flow can lead to ureteric necrosis, a serious complication.
Nerve Supply of the Ureter
Autonomic Innervation
The ureter receives both sympathetic and parasympathetic innervation:
- Sympathetic fibres: Originate from the T10–L2 spinal segments. These fibres are involved in the regulation of ureteric peristalsis and vasoconstriction.
- Parasympathetic fibres: Arise from the pelvic splanchnic nerves (S2–S4), enhancing peristaltic activity.
Pain Pathways
Pain sensations from the ureter are carried via sympathetic afferent fibres to the T11–L2 spinal segments. This explains why ureteric pain (colic) is often referred to the lower abdomen, groin, or genital regions. Nurses must recognise these pain patterns, as they can guide the diagnosis of ureteric pathologies such as stones or infections.
Relevance to Nursing Care
Understanding the nerve supply is essential for pain assessment and management in patients with ureteric conditions. Nurses play a key role in monitoring pain, administering analgesics, and educating patients about referred pain and its implications.
Functions of the Ureter
Transport of Urine
The primary function of the ureter is to transport urine from the renal pelvis to the urinary bladder. This process is continuous and unidirectional, preventing backflow and potential infection.
Peristalsis and Physiological Mechanisms
Peristalsis is the rhythmic contraction of the muscularis layer, propelling urine down the ureter. These contractions occur at a rate of 1–5 per minute and are modulated by autonomic nerves and local reflexes. Peristalsis ensures that urine reaches the bladder efficiently, regardless of body position or gravity.
The ureter’s oblique entry into the bladder wall forms a functional valve, preventing urine from flowing backward (vesicoureteral reflux) when the bladder contracts during micturition.
Clinical Significance of the Ureter
Common Pathologies
- Ureteric Stones (Urolithiasis): Stones can become lodged at the natural constrictions, causing severe pain (renal colic), haematuria, and potential obstruction. Nurses need to monitor for signs of infection, obstruction, and provide pain management.
- Ureteric Strictures: Narrowing of the ureter, often due to injury, surgery, or chronic inflammation, can lead to hydronephrosis and impaired kidney function.
- Ureteric Infections (Ureteritis): Usually secondary to ascending urinary tract infections. Symptoms include dysuria, fever, and flank pain.
- Congenital Anomalies: Conditions such as duplicated ureters or ectopic ureteric insertion may present in childhood and can lead to recurrent infections or incontinence.
- Tumours: Both benign and malignant tumours can affect the ureter, though they are relatively rare.
Symptoms and Diagnostic Approaches
Symptoms of ureteric pathology may include:
- Flank pain or colicky abdominal pain
- Haematuria (blood in urine)
- Fever and chills (if infection is present)
- Difficulty or pain during urination (dysuria)
Diagnostic methods include:
- Urinalysis: To detect infection, blood, or crystals.
- Imaging: Ultrasound, X-ray (KUB), CT scan, or intravenous urography to visualise stones, strictures, or tumours.
- Cystoscopy: Direct visualisation of the lower ureter and bladder.
Nursing Considerations
Assessment and Monitoring
Nurses are at the forefront of assessing patients for ureteric disorders. Key responsibilities include:
- Monitoring vital signs and urine output
- Assessing for pain, location, and pattern
- Observing for signs of infection (fever, chills)
- Checking for haematuria and changes in urine characteristics
- Documenting symptoms and communicating with the healthcare team
Patient Education
Patient education is a vital nursing role. Nurses should inform patients about:
- The importance of hydration to prevent stone formation
- Recognising early signs of infection or obstruction
- Medication adherence and potential side effects
- Post-surgical care if applicable
- Lifestyle modifications for prevention of recurrence
Interventions
Nursing interventions for patients with ureteric conditions may include:
- Pain management (analgesics, antispasmodics)
- Assisting with diagnostic procedures (preparation, post-procedure care)
- Monitoring fluid balance and encouraging oral intake, unless contraindicated
- Administering antibiotics for infections as prescribed
- Supporting post-operative recovery following surgical interventions
Summary and Key Takeaways
For nursing students and professionals, a thorough understanding of the ureter’s anatomy is essential for effective patient care. Key points include:
- The ureter is a muscular tube transporting urine from the kidney to the bladder, measuring roughly 25–30 cm in adults.
- It has three main anatomical constrictions prone to stone impaction.
- Histologically, the ureter comprises mucosa, muscularis, and adventitia, each serving a distinct function.
- Segmental blood supply and autonomic nerve supply are crucial for its function and must be considered during surgical procedures.
- Common ureteric disorders include stones, strictures, and infections, with symptoms often presenting as pain, haematuria, or fever.
- Nurses play a pivotal role in assessment, monitoring, patient education, and intervention for ureteric conditions.
An in-depth knowledge of ureteric anatomy not only enhances clinical skills but also improves patient outcomes through timely recognition, intervention, and education.
REFERENCES
- Ross and Wilson, Anatomy and Physiology in Health and Illness, Fourteenth Edition, 1 July 2022, ISBN-13: 978-0323834612.
- Roger Watson, Anatomy and Physiology for Nurses, 14th Edition, 12-06-2018, ISBN: 9780702077418
- P.R Asha Latha, Text Book of Applied Anatomy & Physiology for Nurses, 7th Edition,3 January 2024, ISBN-13: 978-9356968622.
- Bryan H. Derikson, Tortora’s Principles of Anatomy and Physiology, 16th Edition, August 2023, ISBN: 978- 1119400066.
- Anatomy.co.uk, Reproductive System, Last updated on April 24, 2025, https://anatomy.co.uk/reproductive-system
Stories are the threads that bind us; through them, we understand each other, grow, and heal.
JOHN NOORD
Connect with “Nurses Lab Editorial Team”
I hope you found this information helpful. Do you have any questions or comments? Kindly write in comments section. Subscribe the Blog with your email so you can stay updated on upcoming events and the latest articles.



